
Median Overall survival was nearly doubled among patients with previously treated metastatic pancreatic cancer who received the multiselective RAS(ON) inhibitor daraxonrasib in the phase III RASolute 302 trial, the results of which were presented at the Plenary Session of the 2026 ASCO Annual Meeting by Brian M. Wolpin, MD, MPH, Director of the Hale Family Center for Pancreatic Cancer Research and the Gastrointestinal Cancer Center, Dana-Farber Cancer Institute, Boston.1 These data were simultaneously published by Eileen O’Reilly et al in The New England Journal of Medicine.2
Brian M. Wolpin, MD, MPH

Eileen O’Reilly, MD
Median overall survival was 13.2 months with daraxonrasib vs 6.7 months with chemotherapy (hazard ratio [HR] = 0.40; P = 4.6 × 10-11) in the overall population, which included patients with metastatic pancreatic ductal adenocarcinoma with and without an identified tumor RAS mutation. The Kaplan-Meier curve drew immediate thunderous applause and a rare 42-second standing ovation from attendees at the Plenary Session.
“Daraxonrasib met all primary and key secondary endpoints, with statistically significant and clinically meaningful improvements in overall survival, progression-free survival, objective response rate, and quality of life in patients with previously treated metastatic pancreatic ductal adenocarcinoma,” Dr. Wolpin said. “The results support daraxonrasib as a new standard of care….”
“I’ve heard this study described as a ‘home run.’ I would say it’s much more—it’s a grand slam,” said Julie R. Gralow, MD, FACP, FASCO, ASCO’s Chief Medical Officer and Executive Vice President, who moderated the press briefing at which the results were presented ahead of the Plenary Session.

Julie R. Gralow, MD, FACP, FASCO

Rachna T. Shroff, MD, MS, FASCO
ASCO Expert Rachna T. Shroff, MD, MS, FASCO, Chief of the Division of Hematology/Oncology at the University of Arizona College of Medicine, Tucson, commented at the press briefing that the findings of RASolute 302 are a “gamechanger…, and we don’t commonly use that word in pancreatic cancer. … It literally checks all the boxes with what we think of as relevant, important, and meaningful clinical outcomes. We have honestly never seen a doubling of survival and a 60% reduced risk of death in patients who have already progressed on chemotherapy, [along with] a significant delay in progression [and] a tripling in response. … This is an incredibly impactful study for our patients, and I congratulate and thank the investigators for it.”
Aberrant RAS pathway activation is the key driver of pancreatic ductal adenocarcinoma, with oncogenic RAS mutations identified in at least 90% of cases, most commonly at codon G12. Daraxonrasib is an oral, RAS(ON) multiselective, tricomplex inhibitor of the active, GTP-bound state of mutant and wild-type RAS.
Key Findings
RASolute 302 included 500 patients (median age = 66 years) with metastatic pancreatic ductal adenocarcinoma who had previously received first-line treatment. They were randomly assigned in a 1:1 ratio to receive 300 mg of daraxonrasib daily or the physician’s choice of standard second-line chemotherapy (gemcitabine plus nab-paclitaxel and liposomal irinotecan plus 5-fluorouracil and leucovorin were the two most common). Most patients had tumors with a RAS G12 variant (228 receiving daraxonrasib, 231 receiving chemotherapy). Those without a RAS G12 variant could have tumors with another RAS variant (G13, Q61) or no RAS variant. Follow-up data were provided for a median of 8.5 months.
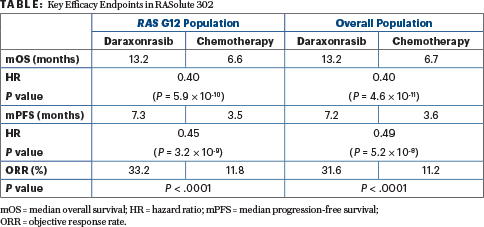
“For our primary endpoint—overall survival in the RAS G12–mutant population—you see a substantial and statistically significant improvement in overall survival for patients in the daraxonrasib arm,” Dr. Wolpin said, as outlined in Table 1. Median overall survival was 13.2 months vs 6.6 months with chemotherapy, with a HR of 0.40 (P = 5.9 × 10-10) and 1-year survival rates of 53.3% and 18.7%, respectively. Median progression-free survival was 7.3 vs 3.5 months, respectively (HR = 0.45; P = 3.2 × 10-9), with 58.7% vs 31.7% of patients, respectively, free of disease progression at 6 months.
“For our key secondary endpoint of overall survival in the overall population [any RAS mutation or none], we saw very similar results,” Dr. Wolpin said (Table 1). Likewise, progression-free survival outcomes appeared to mirror those in the G12 population.
Widespread Benefit: Is Genomic Testing Necessary?
Considering that benefit from the RAS inhibitor was not limited to patients with RAS mutations, would mutation testing be mandatory before prescribing daraxonrasib? Dr. Wolpin advocated for next-generation sequencing regardless.
“Most major consensus guidelines recommend testing for all patients with pancreatic cancer, and my opinion is that we should continue this,” he said at a press briefing. “While RASolute 302 suggests this is an effective therapy in all-comers, there can be rare situations where you may wish to use something else—such as the patient with the occasional RET fusion, in whom I would give a RET-targeted therapy—so I think it’s still appropriate and meaningful to do genomic testing.”
Quality of Life and Safety
“We saw for both pain and global quality of life there was a statistically significant delay to worsening of these features in patients receiving daraxonrasib compared with chemotherapy,” Dr. Wolpin reported.
Median time to deterioration on the pain scale was 9.2 months with daraxonrasib vs 3.8 months with chemotherapy (HR = 0.51; P < .0001) and on the global health status/quality-of-life questionnaire was 5.7 vs 2.6 months, respectively (HR = 0.60; P = .0002).
Grade 3 or higher treatment-related adverse events occurred in 43.6% of the daraxonrasib arm and 57.5% of the chemotherapy arm. Toxicities led to dose reductions in 36.1% and 57.5%, respectively, and to discontinuations in 1.2% of the daraxonrasib arm compared with 11.2% of the chemotherapy arm.
The most common treatment-related adverse events leading to dose reductions were rash (observed in 17.4%) and stomatitis (6.6%). At the press briefing, Dr. Wolpin addressed the concerns about rash: “Rash is by far the most common side effect we see. The majority of patients will get some rash, and most of the time it’s tolerable and we can manage it with appropriate medications. What we have started to do is use a prophylactic strategy, which has been helpful.”
This involves oral antibiotics and topical therapies that can be tapered if rash does not develop or continued and augmented if rash becomes more severe. These topicals typically include hydrocortisone for the face and triamcinolone for the chest and body. Clindamycin and the anti-inflammatory tacrolimus can also be used topically. Some patients may need to pause daraxonrasib to allow time for the rash to improve and then resume treatment, he added.
“As the trial has been running, we have gotten help from our dermatology colleagues to come up with additional strategies,” he continued. “When clinicians start to use the drug, they should have a dermatologist to work with as well, as the rash can be severe in some patients.”
Data from RASolute 302 will be submitted to the U.S. Food and Drug Administration to support its regulatory approval. Daraxonrasib is also being tested as a first-line treatment for pancreatic cancer and as a treatment for other RAS-related cancers.
Editor’s Note: A separate unsolicited but related commentary on this abstract appears here: “Daraxonrasib in KRAS-Mutant Pancreatic Cancer: A First Step in Shifting the Paradigm of Treatment.”
DISCLOSURE: The study was funded by Revolution Medicines. Dr. Wolpin reported personal financial relationships with Agenus, BeiGene (now BeOne Medicines), the Bristol Myers Squibb Foundation, EcoR1 Capital, Harbinger Health, Immuneering, Ipsen, Mirati Therapeutics, Revolution Medicines, Takeda, Tango Therapeutics, and Third Rock Ventures. Dr. Gralow reported no relevant disclosures. Dr. Shroff has served as an advisor or consultant for AstraZeneca, Boehringer Ingelheim, Boston Scientific, Ipsen, and Novocure.
REFERENCES
1. Wolpin BM, Wainberg ZA, Hendifar A, et al: Daraxonrasib, a RAS(ON) multi-selective inhibitor vs chemotherapy in previously treated metastatic pancreatic adenocarcinoma (mPDAC): Primary and final analysis from the phase 3 RASolute 302 study. 2026 ASCO Annual Meeting. Abstract LBA5. Presented May 31, 2026.
2. O’Reilly EM, Wainberg ZA, Hendifar AE, et al: Daraxonrasib or chemotherapy in previously treated metastatic pancreatic cancer. N Engl J Med. Published online May 31, 2026.
EXPERT POINT OF VIEW
Invited discussant Jennifer Knox, MD, MSc, FRCPC, Professor of Medicine at the University of Toronto and a medical oncologist at Princess Margaret Cancer Centre, Toronto, kicked off her comments on RASolute 302 with a broad statement: “The targeting of RAS is a gamechanger for pancreatic cancer. There is unprecedented hope and progress at last. … RAS-targeted therapy should dominate trials across the full spectrum of pancreatic clinical presentations, either as monotherapy or in rational combinations, to impact survival and quality of life and to benefit more patients.”1

Jennifer Knox, MD, MSc, FRCPC
In other words, the success observed with daraxonrasib ushers in a new era. There are now more than 50 RAS inhibitors—some multispecific, like daraxonrasib, and others allele-specific—in clinical development.
Commenting on the notable findings with daraxonrasib, she observed the following about the Kaplan-Meier overall survival curve: “It’s absolutely beautiful. The curves separate early and get wider with time. I don’t think this has ever been seen in pancreatic cancer. A hazard ratio of 0.40 means a 60% less chance of dying at every time point on the curve. Hopefully, with long-term follow-up, we might see a tail on that curve.”
“The other incredibly important finding, especially since it’s pancreas cancer, is the improvement in time to deterioration of pain as a symptom as well as in global quality of life because these patients are so very sick, so it is an unprecedented positive trial,” she continued. “I would argue that the survival, the quality of life, and the pain control are the most important endpoints for our patients, despite the fact that the trial met all its other endpoints as well.”
She acknowledged that she would have preferred to see such an effective new agent evaluated in the first-line setting rather than the second line, as many patients fail to reach second-line therapy. “To introduce probably the most exciting strategy in 5 decades to this smaller population is perhaps the limitation of the study,” she maintained. “However, it was a very pragmatic study and approach; there’s no ideal second-line therapy, you get a faster readout of efficacy, faster potential licensing, and a faster route to more trials and, hopefully, a faster drug to patients—so I accept that, mostly because it’s so positive.”
She acknowledged that toxicity can be a problem, but the median dose intensity remained high and treatment discontinuations were uncommon. The potential for rash and stomatitis is, she said, “a call to action to the oncology community. … We need to optimize supportive care resources to minimize these problems. There are recommendations in place that seem to help if you take preventative measures before you introduce the drug. We can probably build on that, especially if we’re involving our dermatology colleagues.”
In closing, Dr. Knox said, “This is the first glimpse at the real power of targeting RAS in pancreas cancer. I think we have to bring precision medicine right to the front and profile every patient. First-line patients will have the greatest impact. We’ll treat the greatest number, and they’ll probably do better. Imagine being able to treat a frail patient, who can’t start chemotherapy, on a single oral agent. There is the potential to de-escalate challenging combinations by dropping a drug.”
Other studies have shown strong results with daraxonrasib as a single agent and in the front-line setting; evaluations in subgroups and in the adjuvant and even the neoadjuvant settings should be next, she said. “Our ‘future directions’ are really ‘now.’”
DISCLOSURE: Dr. Knox reported personal financial disclosures for Astellas, AstraZeneca, Incyte, Ipsen, and MedImmune.
REFERENCE
1. Wolpin BM, Wainberg ZA, Hendifar A, et al: Daraxonrasib, a RAS(ON) multi-selective inhibitor vs chemotherapy in previously treated metastatic pancreatic adenocarcinoma (mPDAC): Primary and final analysis from the phase 3 RASolute 302 study. 2026 ASCO Annual Meeting. Abstract LBA5. Presented May 31, 2026.