

Muhammad Rafiqul Islam, MBBS, MD
The number of deaths related to breast cancer are increasing at an alarming pace worldwide. According to a World Health Organization (WHO) 2020 report, approximately 2,088,849 new cases and 627,000 deaths related to breast cancer occurred in 2018.1 More than 55% of these deaths occurred in low- to middle-income countries.2
Over the past 40 years, the incidence of breast cancer has increased two- to threefold in East Asian populations. These changes have taken place mainly in urban areas.3 The concept of “fighting for a better living” has driven people toward more urbanization, a widely cited cause of escalating breast cancer numbers in this region. According to the World Bank, Bangladesh experienced faster urbanization than the entire region of South Asia as a whole between 2000 and 2010. Over that period, the share of its population living in officially classified urban settlements increased by 1.69% per year, which is on par with the pace of urbanization experienced by today’s high-income countries in the late 19th century.4
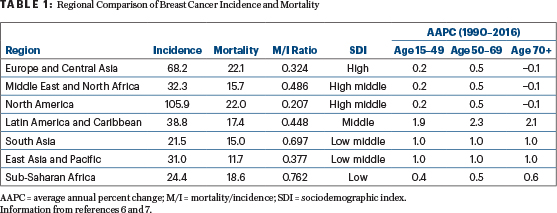
Due to the lack of a robust national cancer registry system in Bangladesh, accurate data for this region, as compared with other parts of the world, are unclear. As a country located in the neighborhood of India (whose breast cancer incidence is 25.8 per 100,000 women5), by extrapolation Bangladesh is expected to see a similar rising trend in the incidence of breast cancer and mortality (Table 1).6,7 Recent data from the cancer registry of the National Institute of Cancer Research & Hospital in Dhaka showed that the breast cancer rate has increased from 26.4% in 2008 to 30.1% in 2017.8,9
Impact of Urbanization on the Incidence of Breast Cancer
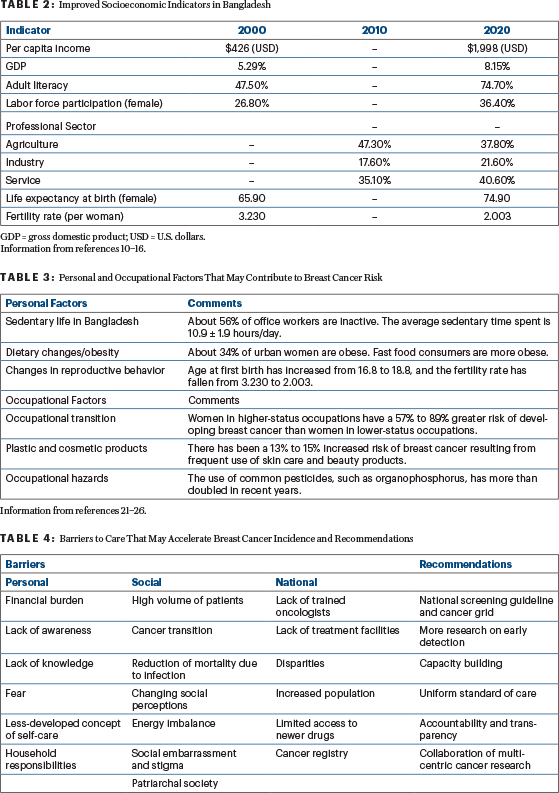
In Bangladesh, per capita income and literacy increased about fivefold and twofold, respectively, in the past 20 years (Table 2).10-16 The age-standardized rate of female breast cancer is positively correlated with the gross domestic product per capita.17 Of note, women with a higher education level seem to have a markedly higher risk of developing breast cancer than women with a lower education level.18
The number of women in the workforce has also increased 38% in the past 20 years. The country’s agriculture-based economy is now shifting to an industry- and service-oriented economy.19,20 Fortunately, as a result of increased access to resources, life expectancy at birth for girls has increased to almost 75 years.15
KEY POINTS
- Recent data from the cancer registry of the National Institute of Cancer Research & Hospital in Dhaka showed that the breast cancer rate in Bangladesh has increased by 26.4% to 30.1% per 100,000 women in the past 10 years.
- Demographic transition and changed lifestyle as well as reproductive practice are adding to the breast cancer incidence in Bangladesh.
- The causes behind the increasing incidence and mortality of breast cancer in low-income countries such as Bangladesh are complex, and solutions will differ from high-income countries.
- There is a need for evidence-based, economically feasible, and culturally appropriate breast cancer screening and treatment guidelines in Bangladesh.
During the past few decades, the rapid uptake of technology, high reliance on electronic communication, and the advent of online activities have led to an overall decrease in physical activity (Table 3).21-27 Moreover, the prevalence of overweight and obesity among Bangladeshi women is increasing due to increased consumption of fast food.28
Furthermore, women living in urban settings are changing their reproductive behavior. Compared with Bangladeshi women living in rural settings, many urban-based women have a lower fertility rate, are delaying childbearing until later in life, have low parity, have a low prevalence of exclusive breastfeeding, and use hormone replacement therapy for many years.23,29-33
The increasing use of pesticides in agriculture and the resultant exposure to them is increasing the chance of developing breast cancer. This is related to the exposure to substances such as malathion, organochlorine terbufos, and chlorpyrifos, all of which have estrogenic potential.26,34 In addition, bisphenol A, an essential component of plastic products, is a possible risk factor for breast cancer. Exposure to plastic products and consumption of food packaged in plastic products is increasing in Bangladesh and potentially increasing the risk of developing breast cancer.35,36 A recent cohort study reported that 13% of these products increased the risk of breast cancer among those who frequently used skin-care products (eg, body lotion, facial cream, hand cream), as well as a 15% increased risk with frequent use of beauty products (eg, foundation, blush, lipstick).25 Evidence has shown that use of skin care and beauty products is increasing in Bangladeshi women.37
Overcoming Challenges
The most cited reason for the increase of breast cancer in low-income countries is “urbanization.” In affluent countries, women are more likely to delay childbearing, reduce breastfeeding, have fewer children, and more frequently use hormone replacement therapy. With urbanization, such behavioral factors are becoming more prevalent in low- to middle-income countries.38 In addition to these issues, low- to middle-income countries have their own unique risk factors that may further accelerate the incidence of breast cancer (Table 4).
Out-of-pocket health-care expenditures from households in Bangladesh account for 64.3% of total health expenditures. Collectively, Bangladeshis have spent approximately 103.46 billion taka (USD = $1.49 billion) from personal funds yearly on health care. This contributes to financial toxicity and pushes almost another 5.8 million people to extreme poverty.39 According to the Hospital Cancer Registry Report 2015–2017 from the National Institute of Cancer Research & Hospital in Dhaka, nearly half (43.5%) of female patients with cancer are illiterate, and 92.8% are housewives.9
Equal educational opportunities and economic freedom for women are necessary for effective breast cancer prevention. Women play a central role in their family, but after a breast cancer diagnosis, many patients in Bangladesh may lose their status in the family; some are divorced or fear divorce because of the disease. As summarized by Fathalla: “Women are not dying because of untreatable diseases. They are dying because societies have yet to decide that their lives are worth saving.”40 Patients who experience more social support and manage their relationships better report healthier outcomes.41 Scarcity of resources and treatment facilities is also contributing to the rising burden and mortality related to breast cancer in this part of the world.
Concluding Remarks
The causes behind the increasing incidence and mortality of breast cancer in low- to middle-income countries such as Bangladesh are complex, and solutions will differ from those in high-income countries. The time is right to take the initiative and develop evidence-based, economically feasible, and culturally appropriate guidelines. The prioritization of biologic and social science research via early detection and the implementation of such research through collaborative, multinational projects will directly impact productivity, prosperity, and quality of life of female patients with breast cancer in Bangladesh.
GUEST EDITOR

Chandrakanth Are, MBBS, MBA, FRCS, FACS
Dr. Islam is an ASCO International Developmental and Education Award recipient and Assistant Professor in the Department of Medical Oncology at the National Institute of Cancer Research & Hospital, Bangladesh.
Acknowledgments: Dr. Islam would like to thank Naoto Tada Ueno, MD, PhD, FACP, of the Department of Breast Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, for modifying this article and improving it significantly. Dr. Islam would also like to thank Professor Nazrina Khatun; A.T.M. Kamrul Hasan, MBBS, MD; and Syeda Masuma Siddiqua, MBBS, MPH, for their enthusiastic encouragement and useful critiques.
REFERENCES
1. World Health Organization: Latest global cancer data: Cancer burden rises to 18.1 million new cases and 9.6 million cancer deaths in 2018. Available at https://www.iarc.who.int/pressrelease/latest-global-cancer-data-cancer-burden-rises-to-18-1-million-new-cases-and-9-6-million-cancer-deaths-in-2018/. Accessed October 5, 2021.
2. Tfayli A, Temraz S, Abou Mrad R, et al: Breast cancer in low- and middle-income countries: An emerging and challenging epidemic. J Oncol. December 15, 2010 (early release online).
3. Porter P: ‘Westernizing’ women’s risks? Breast cancer in lower-income countries. N Engl J Med 358:213-216, 2008.
4. The World Bank: Leveraging urbanization in Bangladesh. September 24, 2015. Available at https://www.worldbank.org/en/country/bangladesh/brief/leveraging-urbanization-bangladesh. Accessed October 5, 2021.
5. Malvia S, Bagadi SA, Dubey US, et al: Epidemiology of breast cancer in Indian women. Asia Pac J Clin Oncol 13:289-295, 2017.
6. Lima SM, Kehm RD, Terry MB: Global breast cancer incidence and mortality trends by region, age-groups, and fertility patterns. EClinicalMedicine 38:100985, 2021.
7. Hu K, Ding P, Wu Y, et al: Global patterns and trends in the breast cancer incidence and mortality according to sociodemographic indices: An observational study based on the global burden of diseases. BMJ Open 9:e028461, 2019.
8. National Institute of Cancer Research & Hospital: Hospital-based Cancer Registry Report 2014. Available at https://nicrh.gov.bd/images/reports/0d08a-hbcr-2014.pdf. Accessed October 5, 2021.
9. National Institute of Cancer Research & Hospital: Hospital Cancer Registry Report, NICRH, Dhaka 2015–2017. December 2020. Available at http://dx.doi.org/10.13140/RG.2.2.10796.08320. Accessed October 5, 2021.
10. Knoema: Bangladesh–Gross domestic product per capita in current prices. Available at https://knoema.com/atlas/Bangladesh/GDP-per-capita. Accessed October 5, 2021.
11. Macrotrends: Bangladesh GDP Growth Rate 1961–2021. Available at https://www.macrotrends.net/countries/BGD/bangladesh/gdp-growth-rate. Accessed October 5, 2021.
12. Knoema: Bangladesh–Adult (15+) literacy rate. Available at https://knoema.com/atlas/Bangladesh/topics/Education/Literacy/Adult-literacy-rate. Accessed October 5, 2021.
13. International Labour Organization: Labor force participation rate, female (% of female population ages 15+) (modeled ILO estimate)–Bangladesh. The World Bank. Available at https://data.worldbank.org/indicator/SL.TLF.CACT.FE.ZS?locations=BD. Accessed October 5, 2021.
14. Statista: Bangladesh: Distribution of employment by economic sector from 2009 to 2019. Available at https://www.statista.com/statistics/438360/employment-by-economic-sector-in-bangladesh/. Accessed October 5, 2021.
15. Knoema: Bangladesh–Female life expectancy at birth. Available at https://knoema.com/atlas/Bangladesh/topics/Demographics/Age/Female-life-expectancy-at-birth. Accessed October 5, 2021.
16. Macrotrends: Bangladesh Fertility Rate 1950–2021. Available at https://www.macrotrends.net/countries/BGD/bangladesh/fertility-rate. Accessed October 5, 2021.
17. Wen D, Wen X, Yang Y, et al: Urban rural disparity in female breast cancer incidence rate in China and the increasing trend in parallel with socioeconomic development and urbanization in a rural setting. Thorac Cancer 9:262-272, 2018.
18. Dong JY, Qin LQ: Education level and breast cancer incidence: A meta-analysis of cohort studies. Menopause 27:113-118, 2020.
19. Lemma AF, Quattri M, Hagen-Zanker J, et al: Bangladesh economic dialogue on inclusive growth. Available at https://asiafoundation.org/wp-content/uploads/2018/11/EDIG-No.4-Strategies-for-inclusive-growth-in-Coxs-Bazar.pdf. Accessed October 5, 2021.
20. International Labour Organization: Understanding the gender composition and experience of ready-made garment workers in Bangladesh. Available at https://www.ilo.org/dhaka/Whatwedo/Publications/WCMS_754669/lang--en/index.htm. Accessed October 5, 2021.
21. Salwa M, Khalequzzaman M, Haseen F, et al: Physical activity among the office executives of Dhaka, Bangladesh: Marium Salwa. Eur J Public Health 26(suppl 1):ckw175.103, 2016.
22. Godinho-Mota JCM, Gonçalves LV, Mota JF, et al: Sedentary behavior and alcohol consumption increase breast cancer risk regardless of menopausal status: A case-control study. Nutrients 11:1871, 2019.
23. National Institute of Population Research and Training and ICF: Bangladesh Demographic and Health Survey 2017–2018: Key Indicators. Available at https://www.dhsprogram.com/pubs/pdf/PR104/PR104.pdf. Accessed October 5, 2021.
24. Pudrovska T, Carr D, McFarland M, et al: Higher-status occupations and breast cancer: A life-course stress approach. Soc Sci Med 89:53-61, 2013.
25. Rylander C, Veierød MB, Weiderpass E, et al: Use of skincare products and risk of cancer of the breast and endometrium: A prospective cohort study. Environ Health 18:105, 2019.
26. Rahman MS, Malek MA, Matin MA: Trend of pesticide usage in Bangladesh. Sci Total Environ 159:33-39, 1995.
27. World Health Organization: Physical activity. November 26, 2020. Available at https://www.who.int/news-room/fact-sheets/detail/physical-activity. Accessed October 5, 2021.
28. Banik R, Naher S, Pervez S, et al: Fast food consumption and obesity among urban college going adolescents in Bangladesh: A cross-sectional study. Obes Med 17:100161, 2019.
29. Rosner B, Colditz GA, Willett WC: Reproductive risk factors in a prospective study of breast cancer: The Nurses’ Health Study. Am J Epidemiol 139:819-835 1994.
30. White MJ, Muhidin S, Andrzejewski C, et al: Urbanization and fertility: An event-history analysis of coastal Ghana. Demography 45:803-816, 2008.
31. Hossain M, Islam A, Kamarul T, et al: Exclusive breastfeeding practice during first six months of an infant’s life in Bangladesh: A country based cross-sectional study. BMC Pediatr 18:93, 2018.
32. Fortner RT, Sisti J, Chai B, et al: Parity, breastfeeding, and breast cancer risk by hormone receptor status and molecular phenotype: Results from the Nurses’ Health Studies. Breast Cancer Res 21:40, 2019.
33. Vinogradova Y, Coupland C, Hippisley-Cox J: Use of hormone replacement therapy and risk of breast cancer: Nested case-control studies using the QResearch and CPRD databases. BMJ 371:m3873, 2020.
34. Yang KJ, Lee J, Park HL: Organophosphate pesticide exposure and breast cancer risk: A rapid review of human, animal, and cell-based studies. Int J Environ Res Public Health 17:5030, 2020.
35. Islam MS: Prospects and challenges of plastic industries in Bangladesh. J Chem Engineer 26:16-21, 2011.
36. Shafei A, Matbouly M, Mostafa E, et al: Stop eating plastic, molecular signaling of bisphenol A in breast cancer. Environ Sci Pollut Res Int 25:23624-23630, 2018.
37. Amreen NA: The economy of the fairness industry. Dhaka Tribune, January 26, 2019. Available at https://www.dhakatribune.com/opinion/special/2019/01/26/the-economy-of-the-fairness-industry. Accessed October 5, 2021.
38. United Nations: World’s population increasingly urban with more than half living in urban areas. July 10, 2014. Available at https://www.un.org/en/development/desa/news/population/world-urbanization-prospects-2014.html. Accessed October 5, 2021.
39. Huq NM, Al-Amin AQ, Howlader SR, et al: Paying out of pocket for healthcare in Bangladesh–A burden on poor? Iran J Public Health 44:1024-1025, 2015.
40. Fathalla MF: Human rights aspects of safe motherhood. Best Pract Res Clin Obstet Gynaecol 20:409-419, 2006.
41. Romeo A, Di Tella M, Ghiggia A, et al: The traumatic experience of breast cancer: Which factors can relate to the post-traumatic outcomes? Front Psychol 10:891, 2019.