
The National Comprehensive Cancer Network® (NCCN®) first introduced the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) in 1996, initially covering eight tumor types. Three decades later, the NCCN Guidelines® span more than 60 tumor types, subtypes, and related clinical topics. At the NCCN 2026 Annual Conference, faculty highlighted updates and new recommendations across a range of malignancies. This roundup summarizes key changes and practice-relevant takeaways from those presentations.
Prostate Cancer
“MDT [metastasis-directed therapy] has become a key topic of conversation for clinicians and their patients with metastatic APMS [androgen pathway modulator–sensitive] prostate cancer, as it is appropriate in certain subsets.”
—Sandy Srinivas, MD
Management of patients with metastatic prostate cancer that is sensitive to an androgen pathway modulator (APMS prostate cancer, also referred to as castration-sensitive prostate cancer) has long since moved beyond the use of androgen-deprivation therapy (ADT) alone. The choice of which therapeutic combination is appropriate for which patient subset has become a central issue. Sandy Srinivas, MD, briefly reviewed the growing assortment of dance partners for ADT in the form of androgen receptor inhibitors, now many targeting molecular alterations, as well as the emerging role for metastasis-directed therapy, which is featured in the 2026 NCCN Guidelines for Prostate Cancer. Dr. Srinivas is Professor of Medicine (Oncology) and, by courtesy, of Urology at Stanford Medicine and Vice Chair of the NCCN panel on prostate cancer.
Among the key 2026 updates for the optimal treatment approach for patients with metastatic APMS prostate cancer, the NCCN Guidelines have incorporated metastasis-directed therapy into the treatment pathway for metachronous oligometastatic androgen pathway modulator–sensitive disease as a treatment option. Along with this addition is a new section on Principles of metastasis-directed therapy and information on suitable subsets of patients for whom this may be an appropriate therapeutic alternative—for example, for metachronous low-volume M1 disease.
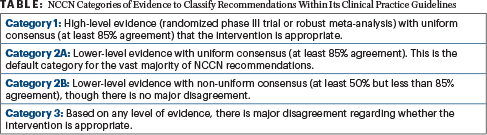
Since seven randomized trials have shown that ADT alone is not adequate for patients with androgen pathway modulator–sensitive disease, Dr. Srinivas noted, the real clinical question becomes which androgen receptor pathway inhibitor (ARPI) should be added to ADT for which patient. Identifying relevant molecular alterations will make this decision clearer. The novel combination of ADT plus the PARP inhibitor niraparib (along with the CYP17 inhibitor abiraterone) has been added to the NCCN Guidelines, and the subsection on PARP inhibitors with late ARPIs has been extensively revised. ADT plus niraparib/abiraterone is considered useful in certain circumstances for synchronous or metachronous high-volume metastases, but only for BRCA2-mutated disease. For low-volume metastases, ADT plus niraparib/abiraterone has been added to the algorithm as a category 2B choice for BRCA2-mutated synchronous or metachronous disease (Table). However, many questions remain surrounding the use of this combination, Dr. Srinivas noted: Is the magnitude of benefit enough, given the absence of an overall survival benefit? Do those with low-volume metachronous disease need it? Is niraparib the best PARP inhibitor in this situation, and how long should patients be on it?
Other additional updates include the replacement of the term “other hormonal agents” with ARPIs throughout the NCCN Guidelines, the addition of a page on “Risk Assessment on Cardiovascular Disease in Prostate Cancer,” and the creation of a table on FDA-Cleared PET Imaging Tracers Studies in Prostate Cancer.
How to integrate the use of PSMA-PET (prostate-specific membrane antigen–positron-emission tomography) imaging for patients with metastatic androgen pathway modulator–sensitive disease has become a challenge, Dr. Srinivas noted. All of the NCCN Guidelines and all of the previous trials have used only conventional imaging, so the results of ongoing trials integrating PSMA-PET imaging are anxiously awaited.
Advanced Renal Cell Carcinoma
“The big challenge is determining subsequent therapy after adjuvant pembrolizumab.”
—Naomi B. Haas, MD
Treatment selection in advanced renal cell carcinoma (RCC) continues to evolve, with several notable updates to the 2026 NCCN Guidelines, according to Naomi B. Haas, MD, Professor of Medicine (Hematology-Oncology) and Director of the Prostate and Kidney Cancer Program at the Abramson Cancer Center at the University of Pennsylvania.
In the updated Guidelines, ipilimumab plus nivolumab has been upgraded from a category 2A to a category 1 preferred first-line regimen for clear cell RCC (ccRCC). In the subsequent therapy setting, lenvatinib was added as a category 2A option useful in certain circumstances for both immunotherapy-naive patients and those previously treated with immunotherapy. Several post-immunotherapy combinations, including axitinib plus pembrolizumab, cabozantinib plus nivolumab, and lenvatinib plus pembrolizumab, were downgraded from category 2A to category 2B recommendations; axitinib plus avelumab was removed as an option.
For non–clear cell RCC, the 2026 Guidelines added a recommendation to consider tumor genomic testing for clinical trial eligibility. “We’re waiting for some of these assays to get a little bit more sensitive, and, hopefully, they will also be helpful,” Dr. Haas noted.
Bladder Cancer
“If we were sitting here 10 or 15 years ago, we likely wouldn’t have a bladder cancer talk because there wouldn’t be much to talk about. We would go for a decade or two without an FDA-approved drug. What a difference the last decade has made.”
—Thomas W. Flaig, MD
Drug approvals over the past decade have reshaped both muscle-invasive bladder cancer (MIBC) and non–muscle-invasive bladder cancer (NMIBC), according to Thomas W. Flaig, MD, Professor of Medicine and Vice Chancellor for Research at the University of Colorado Anschutz Cancer Center, and Charles Peyton, MD, Associate Professor in the Department of Urology, Urologic Oncology, O’Neal Comprehensive Cancer Center, and Director of Clinical Trials at the University of Alabama at Birmingham. Dr. Flaig provided updates in MIBC and Dr. Peyton described new classifications and treatment approaches in NMIBC.
In earlier versions of the NCCN Guidelines for Bladder Cancer, neoadjuvant dose-dense M-VAC (methotrexate/vinblastine/doxorubicin/cisplatin) and gemcitabine/cisplatin constituted the main treatments. This began to change around 5 years ago with the approval of the PD-1 inhibitor pembrolizumab for NMIBC, ushering in the era of immunotherapy. Then in 2023, the antibody-drug conjugate enfortumab vedotin-ejfv was paired with pembrolizumab (EV+P), and this regimen became approved for metastatic urothelial carcinoma.
More recently, KEYNOTE-905/EV-303 addressed patients with MIBC who decline or are ineligible for cisplatin-based chemotherapy—a population that historically proceeded directly to cystectomy. Patients receiving perioperative EV+P achieved a 57% pathologic complete response rate, a 66% downstaging rate, a 60% reduction in risk for an event (P < .001), and a 50% reduction in mortality (P < .001). These results led to the regimen’s approval in 2025 for perioperative treatment in cisplatin-ineligible patients. Current NCCN Guidelines now designate EV+P as the sole preferred first-line regimen for locally advanced or metastatic disease, and data are emerging that could move this approach into the larger population of cisplatin-eligible patients, Dr. Flaig said.
Also in 2025, durvalumab with gemcitabine and cisplatin, the NIAGARA regimen, was approved for perioperative treatment with cystectomy and is the preferred treatment for cisplatin-eligible patients. Immune checkpoint inhibitors (durvalumab, pembrolizumab, nivolumab, atezolizumab, avelumab) are now integrated into a number of regimens recommended for different circumstances, and category 1 evidence underpins recommendations for their adjuvant use, a marked upgrade from the meta-analytic inference of the past.
Whereas the pairing of immune checkpoint inhibitors with BCG has biological rationale, toxicity is concerning, and clinical trials have upheld the long-standing support for induction BCG plus maintenance. Radical cystectomy remains the preferred option for many patients with BCG-non-responsive disease, but new agents are emerging: a non-replication adenoviral vector-based gene therapy, nadofaragene firadenovec-vncg, and an interleukin-15 (IL-15) receptor agonist immunotherapy, nogapendekin alfa inbakicept-pmln, are listed as “other recommended” options in BCG-unresponsive NMIBC.
In NMIBC, Dr. Peyton reminded listeners that a risk stratification framework underpins all treatment decisions. High-risk disease is defined by the presence of carcinoma in situ, T1 disease, or Ta tumors that are either greater than 3 cm or multifocal. The classification of patients now also includes BCG-intolerant patients and BCG-exposed patients who have experienced a latent period after BCG before recurrence. The population attracting the most intense drug development is those classified as BCG-unresponsive.
Colorectal Cancer
“Molecularly directed therapies are finally emerging for those with early-stage colorectal cancer.”
—Jeffrey Meyerhardt, MD, MPH, FASCO
The treatment landscape for colorectal cancer has become more molecularly driven and personalized, resulting in more therapeutic options and better prognosis for early-stage patients, according to Jeffrey Meyerhardt, MD, MPH, FASCO, Chief Clinical Research Officer, Douglas Gray Woodruff Chair in Colorectal Cancer Research, Senior Physician at Dana-Farber Cancer Institute, and Professor of Medicine at Harvard Medical School.
Dr. Meyerhardt covered several significant updates now embedded in the NCCN Guidelines: the use of aspirin in PIK3CA-altered tumors, the incorporation of immunotherapy for mismatch repair–deficient tumors, and structured exercise as a guideline-recommended adjunct to treatment. “With these additions,” he said, “the approaches to treat nonmetastatic colorectal cancer are beginning to become more personalized and options have expanded.”
Aspirin has been formally incorporated into the management of patients harboring PIK3CA pathway alterations. Patients with stage II and III colorectal cancer and those with stage 1 rectal cancer who have somatic PIK3CA pathway alterations should start aspirin 100–162 mg daily after recovering from surgery and continue for 3 years. This recommendation also triggered a corresponding guideline recommendation for molecular profiling of all stage II and III colorectal tumors.
Based on the impactful ATOMIC trial of 2025, the Guidelines now list FOLFOX (fluorouracil/oxaliplatin/leucovorin) or CAPOX (capecitabine/oxaliplatin) plus atezolizumab as a preferred regimen for patients with deficient mismatch repair (dMMR) or microsatellite instability-high (MSI-H) stage III colon cancer, with the benefit assumed to extend to patients with POLE/POLD1 mutations and hypermutated phenotypes.
For locally advanced dMMR colon tumors and for rectal cancer, the data on neoadjuvant immunotherapy have been remarkable; in rectal cancer, some patients may avoid surgery entirely. These findings have translated directly into NCCN guidance: checkpoint inhibitor–based neoadjuvant therapy is now the primary pathway to consider for patients with dMMR rectal tumors.
Further, all patients completing adjuvant therapy are now formally advised to begin a structured exercise routine with a goal of at least 150 minutes of moderate-to-vigorous activity weekly, which has been shown to reduce deaths and recurrences by 28%.
Esophageal and Esophagogastric Junction Cancers
“These are incredibly heterogeneous tumors, at the onset and throughout their treatment. And that just adds to the challenge.”
—Mary F. Mulcahy, MD
Gastric, esophageal, and gastroesophageal junction (GEJ) cancers pose formidable challenges for the oncology provider. Tumor biology is complex, patient populations are heterogeneous, and the therapeutic toolkit is rapidly expanding, said Mary F. Mulcahy, MD, Director of Ambulatory Oncology and Associate Director of Operations at the Robert H. Lurie Comprehensive Cancer Center, Director of the Gastrointestinal Oncology Program, and Professor in the Department of Hematology/Oncology, Radiology, and Surgery at Northwestern University. Dr. Mulcahy discussed the use of perioperative and adjuvant systemic therapy, including the expansion of immunotherapies and biomarker-directed therapeutics, from the NCCN Guidelines for Esophageal and Esophagogastric Junction Cancers.
She noted that the molecular landscape now defines the initial workup of these tumors. Comprehensive biomarker profiling, including immunohistochemistry for HER2, PD-L1, and mismatch repair status, as well as molecular and cytogenetic testing for HER2 amplification, BRAF mutational status, microsatellite instability status, and Claudin 18.2 expression, is now recommended regardless of stage, as the expression of such factors helps guide treatment. For example, the distinct Claudin 18.2 high-expressing subgroup is most likely to respond to emerging Claudin 18.2 targeted agents such as zolbetuximab-clzb, which was approved by the U.S. Food and Drug Administration in October 2024. (Other Claudin 18.2–targeted agents are under investigation.)
For medically fit patients with resectable esophageal, GEJ, or gastric adenocarcinoma, perioperative systemic chemotherapy is the Guideline-recommended standard. The FLOT regimen (fluorouracil/leucovorin/oxaliplatin/docetaxel) has established itself as the preferred backbone. Recently, the Matterhorn study evaluated the addition of durvalumab to perioperative FLOT in gastric and GEJ adenocarcinoma and found improved event-free survival with the combination (HR, 0.71; P < .001), although the benefit was less clear in some subgroups.
In patients with both adenocarcinoma and squamous histologies, CheckMate 577 evaluated adjuvant nivolumab in patients with resected esophageal or GEJ cancer who had received neoadjuvant chemoradiotherapy (commonly carboplatin/paclitaxel [CROSS regimen]) and had residual disease at surgery. Disease-free survival was improved with nivolumab across all comers (HR, 0.69; P < .001), with most benefit seen in squamous cell histology and esophageal cancer. Updated overall survival data presented at the 2025 ASCO Annual Meeting, however, failed to reach statistical significance (HR, 0.85; P = .1064), raising questions about the ultimate value of this regimen, she said.
Under current NCCN Guidelines for early-stage disease, adjuvant nivolumab is reserved for patients who received neoadjuvant chemoradiation and have residual disease at resection, a setting that predominantly applies to squamous cell carcinoma. Preoperative chemoradiation has largely been supplanted by perioperative FLOT for adenocarcinoma, and postoperative nivolumab is therefore not typically applicable in that context.
In the population of patients with HER2-positive tumors, KEYNOTE-811 demonstrated the benefit of adding pembrolizumab to trastuzumab plus chemotherapy in PD-L1–expressing tumors, ushering in a new first-line standard. For patients who progress on trastuzumab-containing therapy, fam-trastuzumab deruxtecan-nxki (T-DXd) has been incorporated into the Guidelines as a second-line option, based on the improvement in overall survival in DESTINY-Gastric04.
Three PD-1 inhibitors (nivolumab, pembrolizumab, and tislelizumab-jsgr) have now demonstrated benefit in the first-line metastatic adenocarcinoma setting when added to fluoropyrimidine/platinum chemotherapy. Zolbetuximab has shown clinical benefit when added to fluoropyrimidine/platinum chemotherapy, but its role in the treatment algorithm remains unclear.
For squamous cell carcinoma of the esophagus, the treatment algorithm is comparatively streamlined. Preoperative chemoradiation remains the preferred neoadjuvant approach, and adjuvant nivolumab is indicated for those with residual disease after resection. In the metastatic setting, PD-L1 expression directs therapy.
Agents on the horizon include zanidatamab-hrii, a bispecific IgG antibody targeting two distinct HER2 epitopes, and bemarituzumab, an FGFR2b inhibitor representing a novel pathway target under investigation in gastric and GEJ cancers.
New Guidelines Debuted for Appendiceal Neoplasms
“Appendiceal cancer is not one disease. It’s a collection of many diseases, and it takes all of us trying to figure out what type it is before you treat the patient.”
—Stacey A. Cohen, MD
Appendiceal cancer is rare, occurring in fewer than one per 100,000 individuals, but its incidence is rising, particularly among younger individuals. This trend mirrors a broader epidemiological shift seen in colorectal cancer and carries its own distinct diagnostic and therapeutic challenges, said Stacey A. Cohen, MD, a gastrointestinal oncologist and Professor at Fred Hutch Cancer Center and the University of Washington.
Dr. Cohen delivered a comprehensive overview of current standards and evolving practices in appendiceal cancer care, drawing on the newly published first edition of the NCCN Guidelines for Appendiceal Neoplasms and Cancers. Previously, recommendations for appendiceal tumors were included within the NCCN Guidelines for Colon Cancer, with few recommendations specific to appendiceal cancer. The new Guidelines represent the panel’s acknowledgment of this disease as a unique entity with a spectrum of histologic subtypes requiring specific recommendations for treatment. The underlying principle of histologic precision before therapeutic action is the foundation of clinical care for this disease, she emphasized.
The NCCN Guidelines address the full continuum of care, from diagnosis and histopathologic evaluation through pathologic staging, surgical management, systemic therapy, surveillance, management of recurrent and metastatic disease, and survivorship.
Central to Dr. Cohen’s presentation was the importance of disease classification. Distinctions must be made between appendiceal mucinous neoplasms and true appendiceal adenocarcinomas —two broad categories that differ substantially in behavior, prognosis, and treatment response. Workup should be comprehensive, beginning with colonoscopy and proceeding with imaging and a full tumor marker panel; diagnostic laparoscopy is sometimes warranted in designing a treatment plan. For surgical assessment, two scoring systems are used: the Peritoneal Cancer Index (PCI) and the Completeness of Cytoreduction (CC) score.
For patients with peritoneal metastasis, cytoreductive surgery combined with intraperitoneal chemotherapy (most commonly hyperthermic intraperitoneal chemotherapy), represents the cornerstone of treatment. For patients with adenocarcinoma and peritoneal disease, the timing of surgery relative to systemic therapy is strategically important. Whereas upfront surgery may be appropriate for lower disease burden, the NCCN Guidelines designate neoadjuvant systemic chemotherapy as the preferred approach before cytoreductive surgery for aggressive disease.
Chemotherapy in appendiceal cancer remains an area of significant uncertainty. Adjuvant chemotherapy is generally not given for adenocarcinoma, but may have some benefit in the presence of high-risk features such as nodal involvement, perforation, and peritoneal spread, which herald a much worse prognosis. Surveillance intensity and interval are tailored to tumor biology, reflecting the considerable variation in oncologic outcomes by histologic subtype and stage.
Advanced Cutaneous Melanoma
“[Neoadjuvant and adjuvant therapy, as well as late-line treatment, are] areas where there have been significant changes over the past few years.”
—Douglas B. Johnson, MD, MSCI
A key 2026 update to the NCCN Guidelines for cutaneous melanoma is that neoadjuvant systemic therapy is now the preferred initial approach for patients with resectable nodal disease, a shift from the historical practice of surgery first, according to Douglas B. Johnson, MD, MSCI, Professor of Medicine at Vanderbilt University Medical Center, Co-Leader of the Translational Research and Interventional Oncology Research Program, Clinical Director of Melanoma at Vanderbilt-Ingram Cancer Center, and Vice Chair of the NCCN Guidelines Panel for Cutaneous Melanoma.
Current NCCN Guidelines list pembrolizumab and ipilimumab plus nivolumab as preferred neoadjuvant options, with ipilimumab plus nivolumab carrying a Category 1 designation. Nivolumab alone and nivolumab plus relatlimab-rmbw, an anti-LAG-3 monoclonal antibody, are listed as other recommended regimens, and dabrafenib plus trametinib is considered useful in certain circumstances for patients with BRAF V600–mutated disease, particularly when tumor shrinkage is needed before surgery.
Non-Melanoma Skin Cancers
“Nonmelanoma skin cancer is a disease that oftentimes does not get as much love as melanoma but certainly warrants a lot of attention.”
—Vincent T. Ma, MD
Recent updates to the NCCN Guidelines and emerging clinical trial data are refining the management of cutaneous squamous cell carcinoma (cSCC) and informing surveillance strategies in Merkel cell carcinoma, according to Vincent T. Ma, MD, Assistant Professor at the University of Wisconsin School of Medicine and Public Health.
In unresectable, advanced-stage, and metastatic cSCC, anti–PD-(L)1 therapies are considered the standard of care for most patients. “We have a variety of different flavors from which we can choose,” Dr. Ma noted, including cemiplimab-rwlc, pembrolizumab, and cosibelimab-ipdl, all FDA-approved, with response rates in the 40% to 50% range and evidence of durability. Adjuvant cemiplimab-rwlc has now been incorporated into the NCCN Guidelines as a Category 1 preferred recommendation for patients with extremely high-risk nodal and non-nodal features following surgery and adjuvant radiation therapy, supported by the phase III C-POST trial, which demonstrated a significant improvement in disease-free survival with adjuvant cemiplimab vs placebo (HR, 0.32). The FDA approved adjuvant cemiplimab for this indication in October 2025. Neoadjuvant cemiplimab-rwlc may also be considered in select patients with very high-risk cSCC, including those with rapidly growing tumors, borderline resectable disease, or tumors for which surgery alone may be unlikely to achieve cure or could result in significant functional impairment.
In Merkel cell carcinoma, active surveillance remains the standard of care following definitive therapy. As of March 2026, there are no FDA-approved adjuvant systemic therapies for definitively treated Merkel cell carcinoma. Tumor-informed circulating tumor DNA (ctDNA) has emerged as a promising surveillance tool, with the NCCN Guidelines now recommending ctDNA testing every 3 months. However, ctDNA is not yet validated to guide systemic treatment decisions.
Cervical Cancer
“We can all be advocates for this [ie, access to care, brachytherapy].”
—Junzo P. Chino, MD, FASTRO
The 2026 NCCN Guidelines for cervical cancer include several updates across systemic and radiation therapy, according to Junzo P. Chino, MD, FASTRO, Associate Professor of Radiation Oncology and Director of Brachytherapy at Duke Cancer Institute and a member of the NCCN Cervical/Uterine Cancers Panel.
For patients with recurrent or metastatic cervical cancer, ipilimumab plus nivolumab has been added as an other recommended second-line or subsequent therapy option, including for small cell neuroendocrine carcinoma of the cervix.
In radiation therapy guidance, intraoperative radiation therapy has been upgraded from a category 3 to a category 2A recommendation. Additionally, more specific guidance has been added for vaginal cuff brachytherapy boost after hysterectomy for positive or close vaginal margins, including recommended dose regimens of 5–6 Gy in two to three fractions to either 0.5 cm depth or the vaginal surface, with a treatment active length of typically the apical 3–4 cm.
Brachytherapy remains a cornerstone of curative-intent treatment for cervical cancer and is one of the few modalities designated as a required component of definitive radiation therapy in the NCCN Guidelines, according to Dr. Chino. He emphasized that attempts to omit or replace brachytherapy have consistently led to worse outcomes, including an approximately 86% increased risk of death when it was not used. He also highlighted advances in image-guided brachytherapy, noting that prospective EMBRACE-I data showed 5-year local tumor control rates exceeding 90%, even in advanced disease.
Despite its proven benefit, the presenter noted that brachytherapy remains underused because of barriers including limited physician training, geographic disparities, patient travel burden, and financial disincentives. Dr. Chino said expanded training, specialized centers, and improved treatment infrastructure will be essential to address these gaps. Referring to advocacy for broader access to brachytherapy as a critical component of cervical cancer care worldwide, he emphasized, “We can all be advocates for this.”
Ovarian Cancer
“I don’t think we should be focused only on the primary debulking part of things. Instead, think about the totality of care for patients: What’s the best package they can get?”
—Shitanshu Uppal, MD, MBA
The 2026 NCCN Guidelines for Ovarian Cancer reflect several meaningful updates across the treatment continuum, according to Shitanshu Uppal, MD, MBA, Chief of Gynecologic Oncology at the University of Michigan Rogel Cancer Center, Director of Gynecologic Oncology Initiatives at the Michigan Oncology Quality Consortium, and a member of the NCCN Ovarian Cancer/Fallopian Tube Cancer/Primary Peritoneal Cancer Panel.
One of the most notable additions is in platinum-resistant recurrent disease, where albumin-bound paclitaxel plus the selective glucocorticoid receptor antagonist, relacorilant, has been added as a preferred regimen for patients previously treated with up to three lines of therapy and prior bevacizumab. Dr. Uppal described the ROSELLA trial, which supported this addition, as representing “a completely new approach in ovarian cancer,” one that targets cortisol-driven chemotherapy resistance rather than DNA repair or cell-surface mechanisms.
Also new in platinum-resistant disease, paclitaxel plus pembrolizumab with or without bevacizumab has been added as a useful-in-certain-circumstances option, limited to patients with PD-L1 combined positive score of at least 1. Dr. Uppal noted that KEYNOTE-B96 marks the first meaningful immunotherapy signal in ovarian cancer, with an overall survival of 18.2 vs 14.0 months in PD-L1–positive disease, a notable result in a population with historically limited options.
The 2026 Guidelines also reflect the narrowing PARP inhibitor landscape. Niraparib, olaparib, and rucaparib have been removed from recurrent-disease therapy sections for both platinum-sensitive and platinum-resistant disease, reflecting limited benefit in biomarker-unselected and homologous recombination–proficient populations. PARP inhibitor use is now more clearly concentrated in maintenance settings and biomarker-defined populations.
Mantle Cell Lymphoma: Updates on Diverging Therapeutic Strategies by TP53 Status
“TP53 is a very important marker of adverse outcomes in patients with mantle cell lymphoma.”
—Ann S. LaCasce, MD, MMSc
Treatment strategies for classical mantle cell lymphoma are increasingly diverging by TP53 status and depth of response, according to presentations by Paolo F. Caimi, MD, Professor of Medicine at the Cleveland Clinic Lerner College of Medicine and Associate BMT and Cell Therapy Director at Cleveland Clinic Cancer Institute, and Ann S. LaCasce, MD, MMSc, Associate Professor of Medicine at Harvard Medical School and a member of the Lymphoma Program at Dana-Farber.
Dr. Caimi focused on newly diagnosed classical TP53 wild-type mantle cell lymphoma, where the historical role of autologous stem cell transplantation (ASCT) in first remission is being actively reassessed. ASCT became a standard consolidation strategy for younger, fit patients, but newer data are challenging its routine use. In the TRIANGLE trial, a BTK inhibitor–containing approach without ASCT produced outcomes comparable to transplant-containing strategies, suggesting that targeted therapy may reduce the incremental value of ASCT for many patients. The EA4151 trial reinforced this finding from a different angle, using MRD to guide treatment decisions: among patients who achieved complete remission with undetectable MRD after induction, ASCT did not improve progression-free or overall survival. The 2026 NCCN Guidelines now reflect this evidence directly: patients achieving complete remission with undetectable MRD (uMRD6) should not receive ASCT, whereas those with detectable MRD (dMRD6) may still be considered for transplant consolidation.
Dr. LaCasce addressed TP53-mutated classical mantle cell lymphoma, a biologically distinct high-risk subgroup in which intensive chemoimmunotherapy and transplant have not consistently overcome poor outcomes. She emphasized that TP53 sequencing (rather than immunohistochemistry alone) is needed to properly define this risk group, and that approximately 10% of newly diagnosed patients harbor TP53 mutations, with prevalence rising substantially in the relapsed setting.
For TP53-mutated disease, novel combinations are becoming more relevant than traditional treatment intensification. The BOVen regimen (zanubrutinib/obinutuzumab/venetoclax) has shown encouraging activity with a 2-year progression-free survival rate of 72%, though follow-up remains short and the regimen may not be ideal for highly proliferative or blastoid disease. The 2026 Guidelines also add acalabrutinib plus rituximab as an option for patients with TP53-mutated disease who are not suitable for aggressive induction therapy.
In relapsed and refractory disease, the updated Guidelines now separate recommendations by whether patients are covalent BTK inhibitor–naive or have experienced late relapse vs those with progression on or early relapse after a covalent BTK inhibitor, a clinically meaningful distinction given that outcomes after BTK inhibitor failure remain poor. Newer options in this setting include the bispecific CD20-directed CD3 T-cell engager, mosunetuzumab-axgb, plus the CD79b-directed antibody-drug conjugate, polatuzumab vedotin-piiq, which has shown activity including in TP53-mutated or -deleted disease, and glofitamab-gxbm, a CD20-directed CD3 T-cell engager. Both of these regimens are reflected in the updated Guidelines.
Together, the presentations underscored a major shift in mantle cell lymphoma: treatment is moving away from uniform intensification and toward biologic and response-adapted care.
Relapsed/Refractory Multiple Myeloma
“The area of relapsed myeloma has significantly changed. We have the initial relapses, the first and second relapse, where we have lots of options. When we get to relapse three and four, those options certainly dwindle, but we still have quite a few exciting new therapies that are coming along in clinical trials that we can continue to apply to these patients who need therapy, relapse after relapse.”
—Shaji K. Kumar, MD
Treatment selection in relapsed or refractory multiple myeloma has become increasingly complex, with expanding options across early and later relapses, according to Shaji K. Kumar, MD, Professor of Medicine at Mayo Clinic Comprehensive Cancer Center in Rochester, Minnesota.
In earlier relapse, the 2026 NCCN Guidelines now include the CD38–targeted monoclonal antibody, daratumumab, plus teclistamab-cqyv, a bispecific B-cell maturation antigen (BCMA)-directed CD3 T-cell engager, as a category 1 preferred regimen for patients with bortezomib- and lenalidomide-refractory disease after one prior therapy including lenalidomide and a proteasome inhibitor. This addition was supported by the phase III MajesTEC-3 trial, which showed a substantial progression-free survival benefit with teclistamab plus daratumumab compared with daratumumab-based standard regimens: 83.4% vs 29.7% at 36 months.
Belantamab mafodotin-blmf, a BCMA-directed antibody drug conjugate, has also reemerged in combination strategies. The Guidelines now list belantamab mafodotin with bortezomib and dexamethasone as a category 1 other recommended regimen after two prior therapies including a proteasome inhibitor and an immunomodulatory drug, supported by data from the DREAMM-7 trial.
For later relapses, linvoseltamab-gcpt, a BCMA-directed CD3 bispecific antibody, has been added as a preferred option after at least four prior lines of therapy, including an anti-CD38 monoclonal antibody, a proteasome inhibitor, and an immunomodulatory drug. Additionally, a new footnote notes that talquetamab-tgvs, a bispecific antibody targeting GPRC5D and CD3, may be considered as a bridge to BCMA-directed CAR T-cell therapy in relapsed or refractory disease.
DISCLOSURES
Dr. Srinivas has served as a scientific advisor to General Electric; Janssen Pharmaceutica Products, LP; Merck & Co., Inc.; Novartis Pharmaceuticals Corporation; and Telix Pharmaceuticals Limited and has received grant/research support from Novartis Pharmaceuticals Corporation. Dr. Haas has received consulting fees from Eisai Co., Ltd. Dr. Flaig reported financial relationships with Aurora Oncology, Criterium, and Janssen Pharmaceutica Products. Dr. Peyton has served as a consultant to Janssen Pharmaceutica Products and UroGen Pharma. Dr. Meyerhardt had no relevant disclosures. Dr. Mulcahy reported no conflicts of interest. Dr. Cohen reported personal financial relationships with AbbVie, Boston Scientific, Caris Life Sciences, Delcath Systems, Eisai, Exact Sciences, GSK, Hexagon Bio, Incyte, and Merck. Dr. Johnson has served as a scientific advisor for AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Merck, Novartis, Pfizer, Teiko, and Therakos; and has received grant/research support from Bristol Myers Squibb and Incyte. Dr. Ma has served as a scientific advisor for Bristol Myers Squibb, Delcath Systems, Incyte, IDEAYA Biosciences, Immunocore Holdings, and Regeneron; and has received consulting fees from Bristol Myers Squibb, Delcath Systems, IDEAYA Biosciences, Immunocore Holdings, and Regeneron. Dr. Chino has received consulting fees from KORTUC Inc., LadeRx LLC, and Teleflex Inc. Dr. Uppal reported no conflicts of interest. Dr. Caimi has received consulting fees from AbbVie and Arvinas and has served as a scientific advisor for ADC Therapeutics, Bristol Myers Squibb, Luminary Therapeutics, and Novartis Pharmaceuticals Corporation. Dr. LaCasce has received consulting fees from Kite Pharma, Caribou Biosciences, Genmab A/S, and Pierre-Fabre Pharmaceuticals and has received honoraria from Takeda Pharmaceuticals North America. Dr. Kumar has received grant/research support from AbbVie, Amgen, Bristol Myers Squibb, CARsgen Therapeutics, GSK, Janssen Pharmaceutica Products, Oricell Therapeutics, Regeneron Pharmaceuticals, Roche Laboratories, Sanofi-Aventis U.S., and Takeda Pharmaceuticals North America; has received consulting fees from BD Biosciences, BioLineRx, and Moderna; and has served as a scientific advisor for AbbVie, Amgen, Bristol Myers Squibb, GSK, Janssen Pharmaceutica Products, Regeneron Pharmaceuticals, Roche Laboratories, Sanofi-Aventis U.S., and Takeda Pharmaceuticals North America.