
“Don’t be afraid to give up the good to go for the great.”
— John D. Rockefeller
The ASCO Post is pleased to present Hematology Expert Review, an ongoing feature that quizzes readers on issues in hematology. In this installment, Syed Ali Abutalib, MD, and L. Jeffrey Medeiros, MD, explore the presentation and pathology of Rosai-Dorfman disease (RDD). For each quiz question that follows, select the one best answer. The correct answers and accompanying discussions appear below.
GUEST EDITORS

Syed Ali Abutalib, MD

L. Jeffrey Medeiros, MD
Dr. Medeiros is Professor and Chair, Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston.
Question 1
Which of the following statements about RDD is correct?
A. It can have a widely variable clinical presentation.
B. An infectious agent has been identified in the majority of cases.
C. It is associated with autoimmune disease but not with malignant or hereditary disease.
D. Noncutaneous RDD is more common in older adults.
E. Extranodal disease is present in approximately 70% of patients.
Question 2
Which of the following statements about RDD and associated conditions is correct?
A. Histologic features of RDD have been observed in patients with Hodgkin and non-Hodgkin lymphomas, where lymphoma and RDD can either precede or follow each other or occur in the same lymph node.
B. RDD coexists with an immunologic disease in 10% of cases.
C. The most recent classification of histiocytosis recommends evaluating the IgG4/IgG ratio in all patients with RDD.
D. Germline mutations in the SLC29A3 gene have been reported in patients with familial RDD.
E. All of the above
Question 3
Which of the following statements about the pathology of RDD is correct?
A. Involved lymph nodes show marked sinusoidal expansion with proliferation of large histiocytes within the sinuses.
B. Nodal RDD is often accompanied by numerous polyclonal plasma cells.
C. Emperipolesis is a helpful finding but is not required for diagnosis.
D. The immunophenotype of the large RDD histiocytes is characterized by cytoplasmic and nuclear S100 and fascin positivity, with CD68 and variable CD163 and CD14 positivity.
E. All of the above
Answers to Hematology Expert Review Questions
Question 1
Which of the following statements about RDD is correct?
Correct answer: A. It can have a widely variable clinical presentation.
Expert Perspective
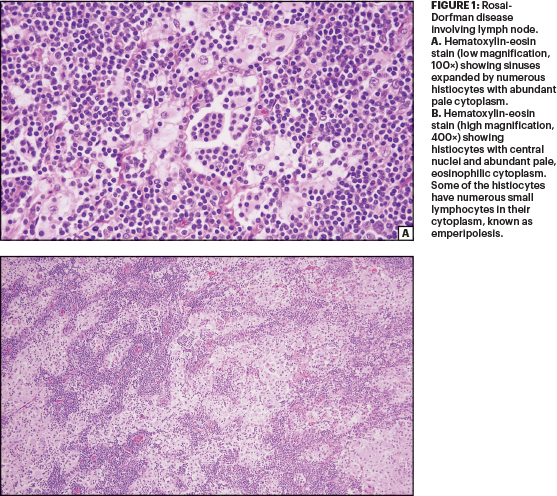
Rosai-Dorfman disease (RDD)—or sinus histiocytosis with massive lymphadenopathy—is a proliferative disorder of histiocytes with distinctive morphologic features. These histiocytes each have a central hypochromatic nucleus, a central distinct nucleolus, and abundant pale cytoplasm. Some of the RDD histiocytes show intracytoplasmic engulfment (trafficking) of small lymphocytes, also known as emperipolesis. These histiocytes are S100 protein–positive (Figure 1). The etiology of RDD is unknown, but a subset of cases have gene mutations involving the MAPK/ERK pathway.1-3
RDD can exhibit a widely variable clinical presentation and can occur as an isolated disorder or in association with other immunologic/autoimmune diseases (eg, asthma, juvenile arthritis, autoimmune hemolytic anemia, systemic lupus erythematosus), neoplasms (eg, non-Hodgkin lymphoma, classical Hodgkin lymphoma), or familial disease (with the SLC29A3 gene implicated).1,2 The etiology of RDD is not well defined and is likely not uniform across the spectrum of phenotypes.
A subset of RDD cases is now recognized to be characterized by recurrent MAPK pathway–activating mutations. An infectious etiology has long been suspected based on the clinical and pathologic manifestations of RDD, but no definitive link with a microorganism has been identified. RDD can be associated with neoplastic diseases, particularly lymphomas, and further research is needed to investigate the cell of origin of the neoplastic types of RDD.
The most common clinical presentation of RDD is chronic, painless massive lymphadenopathy, usually involving cervical lymph nodes and, less frequently, axillary, hilar, peritracheal, and inguinal nodes with or without intermittent fevers, night sweats, and weight loss (ie, B symptoms). Extranodal disease is present in approximately 30% to 40% of patients, with multisystem involvement present in 15% to 30% of patients. Skin involvement (painless, nonpruritic nodules, plaques, or papules) is present in 10% of extranodal RDD cases, though it is rarely isolated and is more common in adults than children (median age = 45 years). However, noncutaneous RDD is more common in children and young adults (median age = 20 years).1,2
Question 2
Which of the following statements about RDD and associated conditions is correct?
Correct answer: E. All of the above.
Expert Perspective
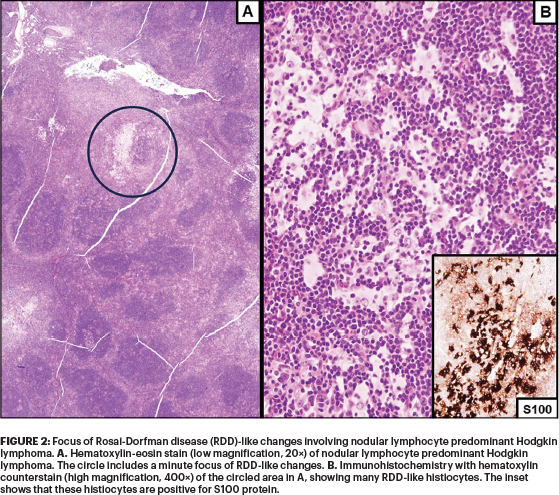
Choices A, B, C, and D are all correct. Additionally, RDD has been reported after myelodysplastic syndrome or bone marrow transplantation for acute leukemia, concurrent with cutaneous clear cell sarcoma, and concurrent with or following L-group histiocytoses or malignant histiocytosis.1 Small foci of RDD-like histopathology (ie, histiocytes with emperipolesis) can occur in association with malignant neoplasms and have not been shown to be clinically important (Figure 2); therefore, some investigators suggest that more than 10% of a specimen involved by RDD morphology is required to constitute a neoplasia-associated RDD rather than a reactive process.1-3
RDD coexists with an immunologic disease in 10% of cases. Some types of extranodal RDD have been associated with an increased number of immunoglobulin G4–positive (IgG4+) plasma cells, although other studies have shown a low number of IgG4+ plasma cells and low IgG4/IgG ratios (< 40%) as compared with IgG4-related disease samples. The SLC29A3 disease spectrum includes familial or Faisalabad histiocytosis, H syndrome, and pigmented hypertrichotic dermatosis with insulin-dependent diabetes, all described as histiocytosis-lymphadenopathy plus syndrome (#602782 in the Online Mendelian Inheritance in Man compendium).1,2
Question 3
Which of the following statements about the pathology of RDD is correct?
Correct answer: E. All of the above.
Expert Perspective
The diagnostic pathologic features of nodal RDD include expansion of sinuses by large distinctive histiocytes. Mitoses and necrosis are rare. Nodal RDD is often accompanied by numerous polyclonal plasma cells in the medullary cords and around the venules, with varying proportions of IgG4/IgG plasma cells. Emperipolesis (from the Greek for “wandering in and around”)—the trafficking of intact leukocytes, erythrocytes, and plasma cells through the cytoplasm—is a helpful finding but is not required for diagnosis.
The immunophenotype of the large RDD histiocytes is characterized by cytoplasmic and nuclear S100 and fascin positivity, with CD68 and variable CD163 and CD14 positivity (Figures 1 and 2).1,2 RDD histiocytes are negative for CD1a and CD207 in contrast with Langerhans cell histiocytosis.1,2
DISCLOSURE: Dr. Abutalib has served on the advisory board for AstraZeneca. Dr. Medeiros reported no conflicts of interest.
REFERENCES
1. Medeiros LJ: Ioachim’s Lymph Node Pathology, 5th ed, pp 246-451. Philadelphia; Wolters Kluwer; 2021.
2. Abla O, et al: Consensus recommendations for the diagnosis and clinical management of Rosai-Dorfman-Destombes disease. Blood 131:2877-2890, 2018.
3. Garces S, et al: Focal Rosai-Dorfman disease coexisting with lymphoma in the same anatomic site. Mod Pathol 32:16-26, 2019.