

Syed Ali Abutalib, MD

Angela Dispenzieri, MD
POEMS syndrome is a poorly understood and complex paraneoplastic plasma cell disorder characterized by peripheral neuropathy and multisystem involvement, including organomegaly, endocrinopathy, monoclonal plasma cell dyscrasia, and skin changes. Clinical manifestations are thought to result from overproduction of cytokines or particularly elevated vascular endothelial growth factor, rather than from relatively low tumor burden.
POEMS syndrome is rare and frequently underrecognized due to its heterogeneous presentation and overlap with other plasma cell–associated and inflammatory disorders. It is a treatable condition, however, and delayed or inaccurate diagnosis is associated with substantial morbidity and mortality. Accurate identification depends on recognizing characteristic clinical patterns and applying established diagnostic criteria.
The following case-based questions focus on key clinical features, diagnostic criteria, and distinguishing characteristics that aid in the accurate diagnosis of POEMS syndrome.
Clinical Vignette
A 62-year-old man presents with a 10-month history of progressive gait difficulty, bilateral foot drop, distal numbness, and increasing difficulty rising from a chair. Neurologic examination reveals symmetric weakness involving ankle dorsiflexion and hip flexion, reduced vibration sense in the feet, and absent Achilles and patellar reflexes. Bilateral lower-extremity edema is noted. There is no bowel or bladder dysfunction.
Laboratory evaluation shows a white blood cell count of 4.5 × 109/L, hemoglobin of 15 g/dL, a platelet count of 550 × 109/L, and a monoclonal gammopathy with a small IgA λ monoclonal protein.
Nerve conduction studies demonstrate a predominantly demyelinating polyneuropathy with mild secondary axonal loss, characterized by prolonged distal latencies, markedly slowed conduction velocities, mildly reduced compound muscle action potential amplitudes, and reduced sensory nerve action potentials.
Question 1
Which of the following characterizations of neuropathy would be most consistent with POEMS syndrome?
A. Symmetric, length-dependent sensorimotor polyneuropathy (predominantly demyelinating)
B. Symmetric, length-dependent sensorimotor polyneuropathy (predominantly axonal)
C. A small fiber neuropathy as determined by epidermal nerve biopsy
D. A and C
Question 2
Which of the following is the most appropriate next diagnostic test to confirm the suspected underlying disorder?
A. Sural nerve biopsy
B. Anti-MAG (myelin-associated glycoprotein) antibody testing
C. Serum vascular endothelial growth factor level
D. Abdominal fat pad biopsy
Question 3
Which of the following statements regarding POEMS syndrome is correct?
A. Adrenal insufficiency is the most common endocrine abnormality
B. Hyperpigmentation is present in nearly all affected patients
C. Extravascular volume overload is a recognized manifestation and occurs in at least one-third of patients
D. Anemia and thrombocytopenia are typical hematologic findings
E. Pulmonary involvement is not associated with this syndrome
Question 4
Which of the following best describes the characteristic bone marrow findings in POEMS syndrome?
A. Sheets of clonal plasma cells with ≥ 10% marrow involvement
B. Lymphoplasmacytic infiltrates
C. Amyloid deposition with variable plasma cell burden
D. Low-level clonal plasma cells with lambda plasma cell rimming of lymphoid
aggregates
E. None of the above
Answers to Hematology Expert Review Questions
Question 1
Which of the following characterizations of neuropathy would be most consistent with POEMS syndrome?
Correct Answer: A. Symmetric, length-dependent sensorimotor polyneuropathy (predominantly demyelinating)
Expert Perspective
This patient’s presentation is characteristic of POEMS syndrome–associated neuropathy, which is best described as a predominantly symmetric, length-dependent demyelinating sensorimotor polyneuropathy. Neuropathy typically begins distally in the lower extremities and progresses proximally, with motor weakness often exceeding sensory loss. Pathologically, POEMS neuropathy is a large-fiber neuropathy associated with endoneurial edema and demyelination, thought to be mediated in part by elevated vascular endothelial growth factor and microvascular dysfunction. Electrophysiologic studies show prominent demyelination, reflected by prolonged distal latencies and markedly slowed conduction velocities, with conduction slowing often disproportionate to the degree of axonal loss. Motor amplitudes are relatively preserved early, consistent with secondary axonal involvement. The presence of a λ light chain–restricted monoclonal protein (most commonly IgG λ or IgA λ) further supports the diagnosis in the appropriate clinical context. Choice C is incorrect because POEMS is not a primary small-fiber neuropathy. Marked small-fiber loss would suggest an alternative diagnosis.
Question 2
Which of the following is the most appropriate next diagnostic test to confirm the suspected underlying disorder?
Correct Answer: C. Serum vascular endothelial growth factor level
Expert Perspective
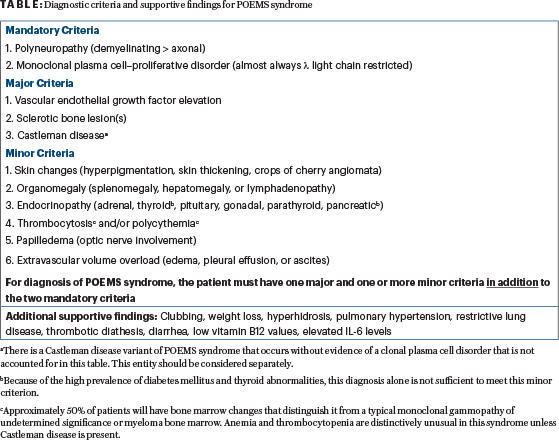
This patient has a symmetric, length-dependent demyelinating sensorimotor neuropathy with early proximal weakness and an IgA λ light chain–restricted monoclonal protein, strongly suggesting POEMS syndrome. Diagnosis requires both mandatory criteria (polyneuropathy and monoclonal plasma cell disorder) plus at least one major criterion (eg, sclerotic bone lesions, Castleman disease, or elevated vascular endothelial growth factor) and one minor criterion (eg, organomegaly, endocrinopathy, skin changes, edema, or papilledema). While vascular endothelial growth factor is a key major criterion, it is not always elevated, so evaluation for other major criteria along with minor criteria should also be performed to secure the diagnosis (Table). Choice B is incorrect because anti-MAG antibody testing is associated with an IgM monoclonal gammopathy and typically causes a slowly progressive, distal sensory–predominant demyelinating neuropathy with minimal proximal weakness, which is not consistent with this patient’s presentation. Choice A is incorrect because sural nerve biopsy is invasive and rarely needed when clinical, electrophysiologic, and laboratory findings strongly suggest POEMS; it is not first-line. Choice D is incorrect because abdominal fat pad biopsy is used to detect amyloid light-chain (AL) amyloidosis, whose peripheral neuropathy is typically a length-dependent small fiber (painful, length-dependent peripheral neuropathy); autonomic dysfunction may also be present.
Question 3
Which of the following statements regarding POEMS syndrome is correct?
Correct answer: C. Extravascular volume overload is a recognized manifestation and occurs in at least one-third of patients
Expert Perspective
Extravascular volume overload is a recognized minor diagnostic criterion in POEMS syndrome and may manifest as refractory peripheral edema, pleural effusions, or unexplained ascites, all of which can contribute substantially to patient morbidity and functional decline, making Choice C correct. Choice A is incorrect because hypogonadism, rather than adrenal insufficiency, is the most common endocrine abnormality in POEMS syndrome. Clinical manifestations frequently include erectile dysfunction, infertility, or early menopausal symptoms. Accordingly, a comprehensive endocrine evaluation is recommended and should include serum testosterone (in males), serum estradiol (in females and males), prolactin, follicle-stimulating hormone, luteinizing hormone, thyroid-stimulating hormone, parathyroid hormone, morning serum cortisol with or without cosyntropin stimulation testing, adrenocorticotropic hormone, and fasting glucose to assess for hypogonadism, thyroid or parathyroid dysfunction, adrenal insufficiency, and glucose intolerance, respectively. Choice B is incorrect because hyperpigmentation, although common, is present in only about half of patients with POEMS syndrome. When present, it typically involves extremities, torso, areola complex, or head and neck, and it may be accompanied by additional cutaneous findings such as acrocyanosis, hypertrichosis, hemangiomas, skin xanthomas, and nail changes. Choice D is incorrect because hematologic abnormalities in POEMS syndrome more commonly include polycythemia and thrombocytosis, whereas anemia and thrombocytopenia are uncommon and usually suggest the presence of concomitant HHV8-negative multicentric Castleman disease or an alternative diagnosis. Choice E is incorrect because pulmonary abnormalities are well recognized in POEMS syndrome and may include pulmonary hypertension, restrictive lung disease, respiratory muscle weakness, and reduced diffusing capacity for carbon monoxide, even though these findings are not incorporated into the formal diagnostic criteria.
In diagnostically challenging cases, ancillary findings—such as reduced diffusing capacity for carbon monoxide (< 70% predicted), elevated right-sided heart pressures (≥ 40 mm Hg), low vitamin B12 levels, thrombotic diathesis, and characteristic nail changes—when interpreted within the appropriate clinical context, can be particularly helpful in reinforcing the diagnosis of POEMS syndrome (Table 1).
Question 4
Which of the following best describes the characteristic bone marrow findings in POEMS syndrome?
Correct Answer: D. Low-level clonal plasma cells with lambda plasma cell rimming of lymphoid aggregates
Expert Perspective
POEMS syndrome is associated with a low-burden clonal plasma cell disorder, most often with λ light chain restriction and typically less than 10% plasma cells in the bone marrow. A distinctive and relatively specific histopathologic feature is plasma cell rimming of lymphoid aggregates, frequently accompanied by megakaryocytic hyperplasia with clustering, which likely explains the common finding of thrombocytosis in these patients. Although this finding is not necessary for a diagnosis, it is not seen in other plasma cell disorders such as monoclonal gammopathy of undetermined significance, AL amyloidosis, or multiple myeloma. Cytopenias are uncommon, which helps to distinguish POEMS from other plasma cell dyscrasias. Choice A is incorrect because sheets of clonal plasma cells with ≥ 10% marrow involvement and lytic bone disease are characteristic of multiple myeloma, not POEMS, which usually shows a low plasma cell burden and sclerotic rather than lytic bone lesions. Choice B is incorrect because Waldenström macroglobulinemia is defined by a lymphoplasmacytic infiltrate producing IgM, often associated with anemia and hyperviscosity, rather than a λ-restricted plasma cell clone with rimming of lymphoid aggregates. Choice C is incorrect because AL amyloidosis is characterized by tissue amyloid deposition with variable plasma cell involvement, a different type of neuropathy, and other organ manifestations such as cardiomyopathy, nephropathy, and/or hepatopathy. The characteristic marrow findings seen in POEMS are not features of AL amyloidosis. Choice E is incorrect because Choice D accurately describes the characteristic bone marrow findings of POEMS syndrome.
DISCLOSURE: Dr. Abutalib reported a financial relationship with AstraZeneca. Dr. Dispenzieri has served as a consultant for Alexion, HemaLogiX, and Janssen, and has received research funding from Pfizer, BMS, Takeda, Alexion, and AbbVie.
SELECTED READINGS
1. Dispenzieri A. POEMS syndrome: diagnosis, treatments, and outcomes. Hematology Am Soc Hematol Educ Program 2025(1):393-400, 2025.
2. Swerdlow SH, Campo E, Harris NL, et al: WHO Classification of Tumours of Haematolymphoid Tissues, 5th ed. Lyon, France: International Agency for Research on Cancer; 2022 (WHO-HAEM5: Plasma cell neoplasms and related paraneoplastic syndromes, including POEMS syndrome).
3. Cook J, Warsame R, Omar M, et al: Interleukin-6 is a highly prognostic biomarker for POEMS syndrome. Leukemia 39(9):2281-2284, 2025.
4. Lee K, Kourelis T, Tschautscher M, et al: Capillary leak phenotype as a major cause of death in patients with POEMS syndrome. Leukemia 39(3):703-709, 2025.
Dr. Abutalib is Director of the Hematologic Malignancies, Hematopoietic Stem Cell Transplantation & Cellular Therapy Program at the Aurora St. Luke’s Medical Center, Milwaukee, Wisconsin. Dr. Dispenzieri is Professor of Medicine at Mayo Clinic College of Medicine and Science, Mayo Clinic, Rochester, Minnesota.