

Stuart Lichtman, MD, FACP, FASCO
The purpose of this editorial is to challenge the continued reliance on Karnofsky Performance Status and Eastern Cooperative Oncology Group (ECOG) or Zubrod performance status as primary tools for evaluating older adults with cancer. These measures have been in oncology practice for decades and are widely used for treatment selection, eligibility determination, and clinical trial stratification. However, evidence demonstrates that they fail to adequately capture the complexity, heterogeneity, and vulnerability of older adults with cancer. I argue that performance status assessments have reached the limits of their clinical usefulness in geriatric oncology and should be replaced, or at a minimum substantially de-emphasized, in favor of systematic geriatric assessment.
Karnofsky and ECOG Performance Status
The Karnofsky Performance Status and ECOG Performance Status scales have long served as the cornerstone of functional assessment in oncology. The Karnofsky Performance Status was introduced in 1948 to evaluate the benefit of nitrogen mustard in lung cancer. It is a physician-rated scale ranging from 0, indicating death, to 100, indicating normal functioning. The ECOG performance status was developed in 1960 as a simplified alternative, measuring functional assessment on a six-point scale from 0, fully active, to 5, death. By the early 1970s, both scales had shifted from tools designed to assess therapeutic benefit to measures used for trial eligibility and stratification.
Their widespread adoption occurred during an era when chemotherapy had a low therapeutic index. Cytotoxic treatments were highly toxic, response rates were modest, and curative potential was limited. In that context, a rapid assessment of patient fitness was reasonable and practical. These scales were simple, intuitive, required no training, and could be completed in seconds. They relied on the physician’s overall impression and intuition on visual assessment of a patient’s overall health or frailty (ie, the eyeball test) and the numerical scale, which allowed for easy documentation and longitudinal comparison.
Despite their convenience, the limitations of performance status assessments are well documented. They are clinician-assessed, inherently subjective, and susceptible to bias. Discrepancies between physician-rated and patient-reported function are common, with patients frequently reporting worse physical function than clinicians assign. Overestimation of performance status may lead to overly aggressive treatment and compromised survivorship, whereas underestimation may deny patients access to beneficial therapies.
The persistence of Karnofsky and ECOG performance status is due to habit and tradition, not because they are the most accurate. The routine reuse of protocol language in clinical trial design has further extended their roles. Meanwhile, the therapeutic landscape has changed dramatically. Treatment benefits are greater, durable responses are more common, and supportive care has improved. Performance status does not capture functional reserve, cognitive impairment, comorbidity, social vulnerability, or frailty. A more precise and individualized approach is required.
Geriatric Assessment
Geriatric assessment is a multidimensional evaluation designed to identify medical, functional, cognitive, psychological, and social vulnerabilities in older adults. In geriatric oncology, it provides critical information not captured by traditional performance measures. Numerous studies demonstrate that even patients categorized as fit by performance status criteria frequently harbor clinically meaningful deficits that influence treatment tolerance and outcomes. There are now multiple randomized trials demonstrating the benefit of geriatric assessment.
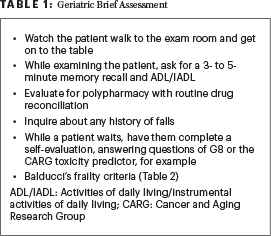
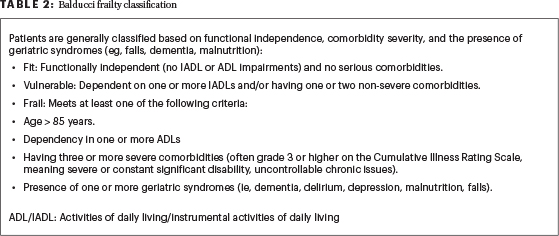
While comprehensive geriatric assessment performed by geriatricians can be time consuming, extensive research demonstrates that abbreviated and focused assessments are feasible in oncology practice and highly predictive. The consistent finding that patients with performance status 0 or 1 harbor meaningful deficits reinforces the necessity of incorporating geriatric assessment into standard care. When time is limited, the accompanying tables show a brief but predictive evaluation (Tables 1 and 2).
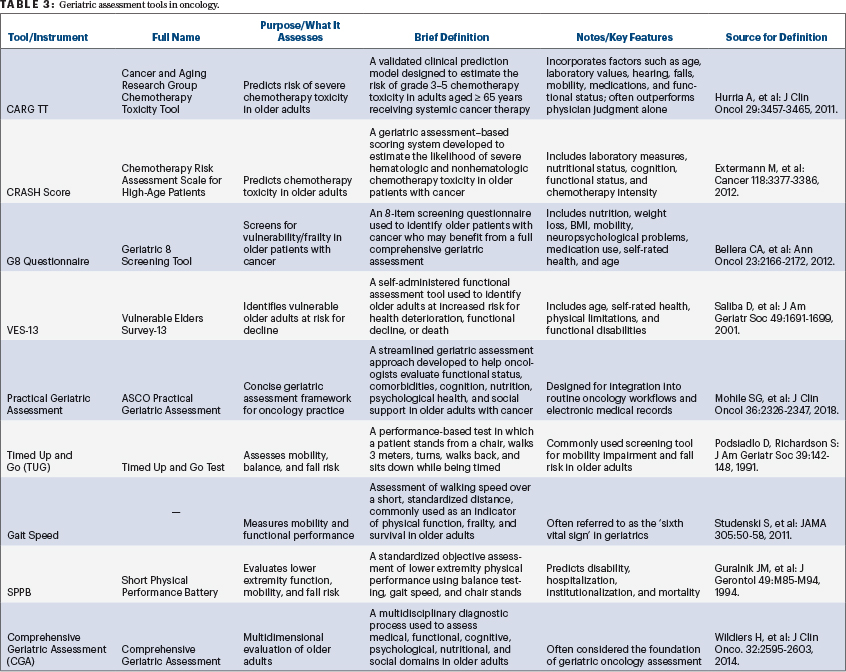
The Cancer and Aging Research Group (CARG) tool and the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score outperform physician judgment in predicting severe chemotherapy toxicity. Additional instruments include the G8 Questionnaire and the Vulnerable Elders Survey. The Practical Geriatric Assessment, developed in collaboration with ASCO, offers a concise and comprehensive framework specifically designed for oncologists, and these tools are being integrated into electronic medical record systems (Table 3).1
The benefits of geriatric assessment are substantial. It has been shown to reduce treatment-related toxicity, preserve quality of life, and maintain independence. It provides essential baseline information and supports evidence-based individualized treatment decisions. Despite this extensive evidence, adoption has been slow. Barriers include time constraints, lack of familiarity, and resistance to change. Ongoing efforts focus on integration into electronic health records and clinician education. Physician education is central to overcoming ageism and treatment bias.
Geriatric assessment is a stronger predictor of chemotherapy toxicity than performance status. Toxicity calculators incorporating geriatric domains outperform physician-rated Karnofsky Performance Status in predicting grade 3 to 5 toxicity. Randomized controlled trials demonstrate that geriatric assessment-directed interventions reduce treatment-related toxicity and premature discontinuation. Individual tests, including instrumental activities of daily living (IADL), nutritional status, and physical performance measures such as Timed Up and Go (a standard clinical screening tool used to assess mobility, balance, and fall risk), gait speed, and Short Physical Performance Battery (objective clinical tool that evaluates lower extremity functioning, mobility, and fall risk), independently predict survival.
Geriatric Syndromes and Their Consequences
Geriatric syndromes further illustrate the shortcomings of performance status. Common syndromes, including frailty, malnutrition, cognitive impairment, depression, polypharmacy, falls, sarcopenia, and reduced social engagement, reflect increased vulnerability to stressors and are often clinically occult even in patients with apparent functional fitness. Their prevalence increases with worsening ECOG performance status, but substantial deficits are common even among patients with preserved performance status. Studies demonstrate high rates of impairment in IADL, cognition, nutrition, and medication burden even among patients with Karnofsky scores of 80 or higher.
These vulnerabilities have significant clinical consequences. They influence prognosis, treatment selection, toxicity risk, and survival. Routine oncology evaluations rarely identify these risks. Falls represent a key example: a history of falls is frequently omitted from standard oncology evaluation and is not reflected in performance status assessments, yet falls are consistently associated with chemotherapy toxicity. The Cancer and Aging Research Group (CARG) toxicity tool is a widely validated clinical calculator used to predict the risk of severe chemotherapy side effects (Grade 3 or higher) in older adults and includes recent falls as a predictor of severe toxicity, and physical performance tests assessing mobility predict survival and early mortality in older patients receiving chemotherapy.
Conclusion
The continued reliance on Karnofsky and ECOG Zubrod performance status as primary assessment tools for older adults with cancer is no longer defensible clinically or ethically.2,3 These measures fail to identify vulnerabilities that meaningfully affect treatment tolerance, toxicity, functional decline, and survival. In contrast, geriatric assessment provides an objective and comprehensive evaluation that reflects the true complexity of older patients. It outperforms performance status and physician judgment in predicting chemotherapy toxicity, postoperative complications, hospitalization, functional decline, and mortality. Randomized trials demonstrate that geriatric assessment-directed interventions reduce severe toxicity, treatment discontinuation, and falls while preserving quality of life and independence.
Concerns regarding feasibility should no longer limit adoption. Brief validated tools can be readily implemented and integrated into electronic health records. The central question is no longer whether geriatric assessment is valuable, but whether continued reliance on outdated tools can be ethically and clinically justified. Geriatric assessment represents the most accurate form of personalized medicine for older adults with cancer. Performance status assessments have reached the limits of their usefulness and should be retired.
DISCLOSURE: Dr. Lichtman reported no conflicts of interest.
REFERENCES
1. Dale W, Klepin HD, Williams GR, et al: Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Systemic Cancer Therapy: ASCO Guideline Update. J Clin Oncol 41:4293-4312, 2023.
2. Lichtman SM: Geriatric assessment is the future: Retiring Karnofsky and ECOG performance status in modern cancer care. Journal of Geriatric Oncology 17:102934, 2026.
3. Lichtman SM: Beyond Performance Status: Optimize Cancer Care in Older Adults. Am Soc Clin Oncol Educ Book 46:e100055, 2026.
Dr. Lichtman is an attending physician (retired) at Memorial Sloan Kettering Cancer Center, Commack, New York; Professor of Medicine at Weill Cornell Medical College, New York; a consultant for Wilmot Cancer Institute Geriatric Oncology Research, University of Rochester; and Past President of the International Society of Geriatric Oncology (SIOG). Dr. Lichtman is also Guest Editor of the Geriatrics for the Oncologist column in The ASCO Post.