
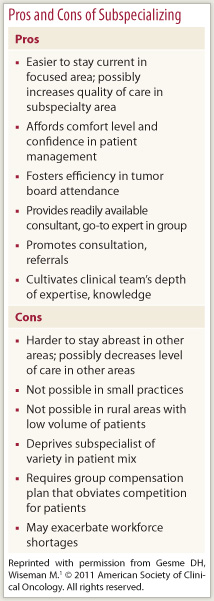
Should oncologists in community practices subspecialize? What would that mean for them and for their patients? These are some of the issues tackled in a Journal of Oncology Practice (JOP) Strategies for Career Success article entitled “Subspecialization in Community Oncology: Option or Necessity?”
What Drives Subspecialization?
 “The pressure that practitioners feel because of the explosion of knowledge in medical oncology has to a great extent driven subspecialization,” wrote Dean H. Gesme, MD, an oncologist with Minnesota Oncology in Minneapolis, and Marian Wiseman, MA, of Wiseman Communications in Washington, DC. “Patients’ growing sophistication has produced pressure, too.”
“The pressure that practitioners feel because of the explosion of knowledge in medical oncology has to a great extent driven subspecialization,” wrote Dean H. Gesme, MD, an oncologist with Minnesota Oncology in Minneapolis, and Marian Wiseman, MA, of Wiseman Communications in Washington, DC. “Patients’ growing sophistication has produced pressure, too.”
In an interview with The ASCO Post, Dr. Gesme said he could easily understand the patient’s perspective. “If I had a personal medical problem, I would certainly want to see someone who had not only a lot of intellectual knowledge, but also a lot of experience dealing with whatever the condition was. Because there is just no substitute for experience in clinical medicine.”
As Larry J. Geier, MD, an oncologist in a large community practice in Kansas City, Missouri, stated in the JOP article, “Patients want this. They want to feel like they are going to someone who really knows their stuff.” Dr. Geier, who specializes in cancer genetics and risk assessment, said that subspecialization improves the quality of care. “If you do it all day every day, you are going to get better and better.”
Generalists Still Needed
 Not everyone thought subspecialization was needed or helpful. “A subspecialist is what the patients need if they happen to have the disease that is specialized in,” stated private oncologist Barbara McAneny, MD, CEO of an Albuquerque, New Mexico, practice with eight medical oncologists. “We need community oncologists who are comfortable taking care of everyone,” she said.
Not everyone thought subspecialization was needed or helpful. “A subspecialist is what the patients need if they happen to have the disease that is specialized in,” stated private oncologist Barbara McAneny, MD, CEO of an Albuquerque, New Mexico, practice with eight medical oncologists. “We need community oncologists who are comfortable taking care of everyone,” she said.
“The need for subspecialization is also made less essential by the ease of internet information searches. While there is no substitute for personal experience, I have found that most experts in unusual tumors are happy to e-mail or talk with us, especially when we have read their papers. Genetically driven personalized medicine will be too much for anyone to keep track of when the field reaches its full potential. I feel that electronic decision support may provide better care than even a referral to a subspecialist,” she said.
 “I certainly feel that there is a very big role for the oncology generalist. There are areas like breast cancer, colon cancer, lung cancer, where all of us who are practicing in the community are going to have to have a modicum of awareness, experience, and scientific knowledge and have to deal with those issues,” Dr. Gesme said. “Most of us need a broad base. And then on top of that, many of us, particularly in large practices, can focus on areas where we have greater depth of knowledge.” He compared it to training in internal medicine before becoming an oncologist. “All of us still use those internal medicine skills to a certain degree,” he said. Subspecialty skills “will be added on top, not necessarily as an alternative to being a generalist or a specialist.”
“I certainly feel that there is a very big role for the oncology generalist. There are areas like breast cancer, colon cancer, lung cancer, where all of us who are practicing in the community are going to have to have a modicum of awareness, experience, and scientific knowledge and have to deal with those issues,” Dr. Gesme said. “Most of us need a broad base. And then on top of that, many of us, particularly in large practices, can focus on areas where we have greater depth of knowledge.” He compared it to training in internal medicine before becoming an oncologist. “All of us still use those internal medicine skills to a certain degree,” he said. Subspecialty skills “will be added on top, not necessarily as an alternative to being a generalist or a specialist.”
Deliberate Departure or Gradual Evolution?
Subspecialization can be a deliberate departure from general oncology—meant to deal with the explosion of knowledge and expectations of patients—or it can evolve, Dr. Gesme said. “Five years ago I talked to my group of physicians and they all agreed they really didn’t want to designate themselves as subspecialists. That was the group think,” Dr. Gesme said. “I look back at this past year and essentially everyone in the group now has some kind of a subspecialty area. We’ve never written it down, but it just evolved that way because we do have a large group and we are actively participating in many different multidisciplinary teams.”
Dr. Gesme’s group includes 59 oncologists throughout the urban Minneapolis area, with 13 oncologists at the site where he practices. “I’ve got some areas that I emphasize, esophageal and head and neck cancer,” he said. “Another physician specializes in melanoma, and many of us, if we have a melanoma patient, will refer the patient to him early on and get his direction. He is very good about sending the patient back. We manage the patient until a specific issue or dilemma arises and then [our melanoma specialist] will again see the patient and help us decide exactly what to do if it is a difficult situation,” he said.
“Whether they embrace subspecialization or lament it, individuals see subspecialization as a growing trend, driven by the increasing complexity of cancer care, the changing delivery systems, and patient demand,” the article concludes. Will that trigger new designations and certifications by professional organizations and specialty societies?
“I think it is premature to do anything immediately,” Dr. Gesme commented, “but I think that is the direction it certainly is going. Studying the issue and being ahead of the curve for professional organizations definitely is something that would make sense.” ■
Reference
1. Gesme DH, Wiseman M: Subspecialization in community oncology: Option or necessity? J Oncol Pract 7:199-201, 2011.