
Patients with smoldering multiple myeloma derived a significant progression-free survival benefit, along with other positive outcomes, from 3 years of subcutaneous use of the monoclonal antibody daratumumab as compared with active monitoring in the phase III AQUILA study.1 These findings were presented at the 2024 American Society of Hematology (ASH) Annual Meeting & Exposition by Meletios-Athanasios Dimopoulos, MD, Professor and Chairman of the Department of Clinical Therapeutics at the National and Kapodistrian University of Athens and Alexandra General Hospital in Greece.

Meletios-Athanasios Dimopoulos, MD
“This is the largest phase III trial conducted in patients with high-risk smoldering myeloma. We believe that with these data, patients with high-risk smoldering myeloma may benefit from immediate treatment with daratumumab and that observation for this particular subset of patients may not be an adequate option,” Dr. Dimopoulos said at a press briefing during the ASH meeting.
There is no approved treatment of high-risk smoldering myeloma, though several large trials have showed that lenalidomide can slow or prevent progression to frank disease.2,3 AQUILA asked whether early intervention could prevent end-organ damage and progression to active myeloma.
After a median follow-up of more than 5 years, median progression-free survival was not reached with daratumumab but was 41.5 months with monitoring. The proportion of patients free of disease progression or death was 63.1% and 40.8%, respectively, a 51% reduction in risk (hazard ratio [HR] = 0.49; P < .001). Benefit was seen across all risk groups, but the benefit was greatest for those at highest risk (HR = 0.36; 95% confidence interval [CI] = 0.23–0.58).
“It was quite interesting to see that while daratumumab was administered for 3 years, there was continuous benefit out to 5 years…, suggesting daratumumab may be altering the natural course of the disease,” Dr. Dimopoulos noted.
AQUILA Details
The open-label randomized study enrolled 390 patients from 124 centers with a duration of smoldering myeloma of up to 5 years; most had intermediate-risk or high-risk disease characteristics. High risk was defined as clonal bone marrow plasma cells ≥ 10% and at least one of these risk factors: serum monoclonal protein level ≥ 30 g/L, IgA disease, immunoparesis with reduced levels of two uninvolved immunoglobulin isotypes, serum involved/uninvolved free light chain ratio ≥ 8 and < 100, or clonal plasma cells in bone marrow of > 50% to < 60%.
Dr. Dimopoulos explained that at the time AQUILA was being designed, these factors were the established criteria for high risk, but today, the Mayo 2018 risk stratification (“20/2/20”) is used (see sidebar). By these Mayo 2018 criteria, in AQUILA, approximately 20% of patients were of low risk, nearly 40% were of intermediate risk, and approximately 40% were considered high risk.
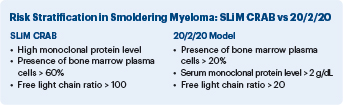
Patients were randomly assigned to active monitoring or receipt of subcutaneous daratumumab at 1,800 mg on a weekly basis in cycles 1 and 2, every 2 weeks in cycles 3 through 6, and every 4 weeks thereafter in 28-day cycles until cycle 39 or disease progression. The primary endpoint was progression-free survival by independent review committee and according to International Myeloma Working Group (IMWG) diagnostic criteria for smoldering myeloma (SLiM CRAB; see sidebar) or death. Following treatment, patients were followed until disease progression by SLiM CRAB criteria.
By data cutoff, 65.5% and 40.8% of patients in the daratumumab and active monitoring arms, respectively, completed 36 months on study. The most common reason for failure was progressive disease (21.8% vs 41.8%, respectively).
Other Benefits With Treatment
Dr. Dimopoulos elaborated on the “robust” benefit in patients deemed at highest risk by the Mayo 2018 criteria, whose risk was reduced by 64%. For these patients, median progression-free survival was not reached, whereas it was 22.1 months in the control arm.
In addition to the significant reduction in risk of disease progression, other benefits were seen with daratumumab treatment vs active monitoring:
- Higher response rate: 63.4% vs 2.0% (P < .0001), with generally consistent improvement across subgroups
- Delayed time to treatment: At data cutoff, 33% of the daratumumab group vs 52% of the monitored group had initiated treatment for active disease. Median time from randomization was not reached with daratumumab and was 50.2 months with active monitoring (HR = 0.46; nominal P < .0001).
- Less disease progression with CRAB criteria: 12 vs 34 patients
- Less disease progression with SLiM criteria: 50 vs 65 patients
- Positive trend for daratumumab in second progression-free survival: a 42% reduction (HR = 0.58; 95% CI = 0.35–0.96)
- Improved overall survival: 60-month rate of 93.0% vs 86.9% (HR = 0.52; 95% CI = 0.27–0.98).
Commenting on fewer patients experiencing disease progression with the SLiM CRAB criteria, Dr. Dimopoulos said: “Not only did daratumumab delay progression, but those patients also avoided a clinically obvious and important type of progression. We saw a benefit across all subsets, but the greatest benefit was for the patients who are at high risk by standard criteria.”
Asked how daratumumab’s benefit stacks up against that reported for lenalidomide in previous studies, Dr. Dimopoulos commented: “The fact that daratumumab is a monoclonal antibody not associated with significant myelosuppression, especially long-standing myelosuppression, and it was given for a limited period, means it is probably a better [single-agent] treatment option…. The benefit appears to be greater, and its limited administration makes it more appealing.”
Safety Profile
Grade ≥ 3 treatment-emergent adverse events were observed in 40.4% of patients in the daratumumab arm compared with 30.1% of those undergoing active monitoring. They were most commonly hypertension (5.7% vs 4.6%, respectively), with pneumonia the most serious (3.6% vs 0.5%, respectively). An increase in infections with daratumumab was noted, but these infections were reported to be reversible. A total of 6.7% discontinued the trial because of adverse events related to daratumumab.
Based on these findings, the manufacturer of daratumumab has submitted a supplemental biologics license application to the U.S. Food and Drug Administration and an extension of indication application to the European Medicines Agency. “I believe it is important to have an approved therapy. Then based on the practice of the physician and the patient, they can make a joint decision whether [the patient] will get the treatment,” Dr. Dimopoulos said.
Expert Point of View
Surbhi Sidana, MD, Associate Professor of Medicine at Stanford University, shared these thoughts with The ASCO Post: “The AQUILA trial in smoldering myeloma remains controversial. On one end, you have a limited duration therapy that is reasonably well tolerated, can prolong time to progression, and can give patients time without developing symptoms of myeloma. On the other hand, the control group had a median time to progression of 4 years…. Are we therefore overtreating some patients?” she asked.

Surbhi Sidana, MD
Despite the benefit shown for lenalidomide in previous studies, “most physicians don’t treat smoldering myeloma, even expert myeloma physicians,” Dr. Sidana noted. “So, what are we actually achieving? If we can cure a proportion, then that moves the needle forward. If we can prevent many patients from developing renal failure or pathologic fractures, that also moves the needle forward…. We need to identify who that subset is—those who will experience disease progression within about 18 months. In those patients, I think we need to intervene.”
According to Dr. Sidana, AQUILA offers “good proof of concept” that intervention is possible, can provide an overall survival benefit, and is not detrimental to patients’ future treatment, but it does not justify treating all patients of the type enrolled in the study. Once those at highest risk are identified, the next question is actually how to treat them, she said. Is single-agent daratumumab sufficient in this precarious group? “Those questions are being asked now in other clinical trials,” she added.
DISCLOSURE: Dr. Dimopoulos reported financial relationships with Sanofi, Regeneron, Manarini, Takeda, GSK, BMS, Janssen, BeiGene, SWIXX, AstraZeneca, and Amgen. Dr. Sidana reported financial relationships with Kite, BMS, Janssen, Sanofi, Oncopeptides, Takeda, Regeneron, AbbVie, Pfizer, BioLineRx, and Legend Biotech.
REFERENCES
1. Dimopoulos MA, Voorhees PM, Schjesvold F, et al: Phase 3 randomized study of daratumumab monotherapy versus active monitoring in patients with high-risk smoldering multiple myeloma: Primary results of the AQUILA study. 2024 ASH Annual Meeting & Exposition. Abstract 773. Presented December 9, 2024.
2. Mateos MV, Hernández MT, Giraldo P, et al: Lenalidomide plus dexamethasone for high-risk smoldering multiple myeloma. N Engl J Med 369:438-447, 2013.
3. Lonial S, Jacobus S, Fonseca R, et al: Randomized trial of lenalidomide versus observation in smoldering multiple myeloma. J Clin Oncol 38:1126-1137, 2020.