
A first-line regimen combining the novel interleukin-2 (Il-2) agonist bempegaldesleukin (NKTR-214) with nivolumab showed encouraging clinical activity in patients with metastatic melanoma in the phase I/II PIVOT-02 trial, according to a presentation during the 2020 Annual Meeting of the Society for Immunotherapy of Cancer (SITC), which was held virtually this year.1 Based on the preliminary results of this study, the combination of bempegaldesleukin and nivolumab was awarded Breakthrough Therapy designation by the U.S. Food and Drug Administration.
Adi Diab, MD, Associate Professor of Melanoma Medical Oncology at The University of Texas MD Anderson Cancer Center, Houston, presented updated data and biomarker analyses at the SITC Annual Meeting, along with results from the phase I REVEAL trial, which also showed promising results for bempegaldesleukin in a variety of solid tumors.2

“NKTR-262 plus bempegaldesleukin led to engagement of the entire immune activation cascade required for systemic tumor clearance.”— Adi Diab, MD
Tweet this quote
“These updated PIVOT-02 clinical data further validate our prior results that bempegaldesleukin plus nivolumab provides both deep and durable responses in the first-line setting of metastatic melanoma,” Dr. Diab said. “We observed a total overall response rate of 53%, with 34% of patients achieving a complete response. Now, we have also observed a median progression-free survival for the entire cohort of 30.9 months.”
Omid Hamid, MD, Chief of Research/Immuno-Oncology at The Angeles Clinic & Research Institute and Co-Director of the Cutaneous Malignancy Program at Cedars-Sinai Cancer Center, Los Angeles, commented: “The complete response rate of 34%...heralds it [the combination] as a possible success.”
Bempegaldesleukin is a CD122-preferential IL-2 pathway agonist shown to increase tumor-infiltrating lymphocytes, T-cell clonality, and PD-1 expression—factors associated with response to immunotherapy. Bempegaldesleukin plus nivolumab has been shown to convert tumors from PD-L1–negative status at baseline to PD-L1–positive status on treatment, according to Dr. Diab.
PIVOT-02: Study Details
The PIVOT-02 trial enrolled 41 patients with previously untreated stage IV melanoma, 38 of whom were evaluable for this analysis. PD-L1 status was known to be positive in 58.5% and negative in 34.1%. Patients received bempegaldesleukin (0.006 mg/kg) plus nivolu-mab (360 mg) every 3 weeks.
The polyfunctional strength index (PSI) of circulating lymphocytes and eosinophil count at baseline and at day 8 of cycle 1 were analyzed using the median cutoff for correlations with response and progression-free survival. Biomarkers, including CD8-positive tumor-infiltrating lymphocytes and interferon-gamma (IFN-g) gene-expression profile, were measured in baseline tumor biopsies and analyzed for correlation with these clinical parameters.
PIVOT-02: Durable Responses Observed
At a median follow-up of 29 months, 20 patients (53%) responded, and 13 of them (34%) were complete responses. Responses were observed regardless of PD-L1 status, in 64% of patients with PD-L1–positive disease, 39% of patients with PD-L1–negative disease, and 33% of patients with an unknown PD-L1 status.
“The responses with bempegaldesleukin plus nivolumab were durable and deepened over time,” Dr. Diab commented.
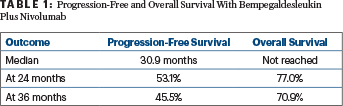
Of the 38 patients, 18 (47%) achieved 100% reduction in target lesions, with 16 (80%) having ongoing responses. The median duration of response had not been reached at a follow-up of 29 months. Median progression-free survival was 30.9 months, and median overall survival had not been reached (Table 1).
“Noninvasive, on-treatment biomarkers predicted response to the combination, well before radiographic evidence,” he said.
There were positive associations between clinical outcomes and the presence of IFN-g profile, CD8-positive tumor-infiltrating lymphocytes, increases in CD4-positive and CD8-positive PSI, and eosinophils.
PIVOT-02: Safety and Tolerability
Grade 3 or 4 treatment-related adverse events were observed in seven patients (17.1%): atrial fibrillation in two (4.9%); acute kidney injury in two (4.9%); and dizziness, dyspnea, hyperglycemia, hypernatremia, and hypoxia in one each (2.4%). Immune-related adverse events grade ≥ 3 were seen in two patients (4.9%). Five patients (12.2%) discontinued bempegaldesleukin or nivolumab due to toxicity. There were no treatment-related deaths.
“We are encouraged by the safety profile and durable responses seen with this combination therapy and look forward to continued evaluation in phase III studies, which are enrolling now,” said Dr. Diab.
REVEAL: Study Details
In the phase I REVEAL trial, 36 patients with advanced refractory solid tumors were treated with the combination of bempegaldesleukin and NKTR-262, a small-molecule agonist of Toll-like receptors. Dr. Diab presented results from the dose--escalation phase.
Given by intratumoral injection, NKTR-262 is retained within the tumor microenvironment and promotes an immunostimulatory milieu and tumor antigen release. Preclinically, NKTR-262 plus bempegaldesleukin combined innate immune signaling and enhanced antigen presentation, with sustained T-cell activation. This resulted in tumor growth inhibition of treated and abscopal lesions.
In the REVEAL trial, patients received escalating doses of NKTR-262 (0.03–3.84 mg intratumorally) followed 3 weeks later by bempegaldesleukin (0.006 mg/kg intravenously); regimens were administered every 3 weeks. The result was early evidence of clinical activity, he said.
REVEAL: Key Findings
Two patients who had experienced disease progression on two prior immunotherapy regimens had partial responses, and five more achieved stable disease, for a disease control rate of 41.2%. Analysis of the immune response revealed increased activation of both T cells and natural killer cells in patients as well as of cytokines and interferon genes, reported Dr. Diab.
“NKTR-262 plus bempegaldesleukin led to engagement of the entire immune activation cascade required for systemic tumor clearance,” he commented.
The most frequent side effects were flu-like symptoms, fatigue, nausea, and itching, all of which are consistent with the known safety profile of bempegaldesleukin. One dose-limiting toxicity of elevated transaminase levels was observed at the highest dosage.
KEY POINTS
- The IL-2 agonist bempegaldesleukin plus nivolumab led to encouraging clinical outcomes in previously untreated patients with stage IV melanoma in the phase I/II PIVOT-02 trial.
- A response rate of 53% was observed, as were a complete response rate of 34% and a median progression-free survival of 30.9 months. Median overall survival has not been reached.
- Bempegaldesleukin plus nivolumab has received Breakthrough Therapy designation.
- In the REVEAL trial, the small-molecule NKTR-262 plus bempegaldesleukin also showed activity in relapsed or refractory melanoma.
Based on these results, bempegaldesleukin plus NKTR-262, with or without nivolumab, will be evaluated in a phase Ib dose-expansion study of patients with relapsed or refractory melanoma (ClinicalTrials.gov identifier NCT03635983).
DISCLOSURE: The studies were supported by Nektar Therapeutics. Dr. Diab has received honoraria from Array BioPharma; has served as a consultant or advisor to Celgene, CureVac, Idera Pharmaceuticals, and Nektar Therapeutics; has received research funding from Apexigen and Merck; has received institutional research funding from Celgene, Idera, Nektar Therapeutics, and Pfizer; and has been reimbursed for travel, accommodations, or other expenses by Nektar Therapeutics. Dr. Hamid has received honoraria from Array BioPharma, Bristol Myers Squibb, Novartis, and Sanofi/Regeneron; has served as a consultant or advisor to Aduro, Akeso Biopharma, Amgen, Array BioPharma, BeiGene, Bristol Myers Squibb, Genentech, GlaxoSmithKline, Immunocore, Incyte, Janssen, Merck, NextCure, Novartis, Regeneron, Roche, Sanofi, Seattle Genetics, Tempus, and Zelluna; has participated in a speakers bureau for Array BioPharma, Bristol Myers Squibb, Novartis, and Sanofi/Regeneron; has received institutional research funding from Aduro Biotech, Akeso Biopharma, Amgen, Arcus Biosciences, Array BioPharma, AstraZeneca, Bristol Myers Squibb, CytomX Therapeutics, Exelixis, Genentech, GlaxoSmithKline, Immunocore, Incyte, Iovance Biotherapeutics, MedImmune, Merck, Merck Serono, Moderna Therapeutics, NextCure, Novartis, Pfizer, Regeneron, Roche, Sanofi, Seattle Genetics, Torque, and Zelluna.
REFERENCES
1. Diab A, Tykodi S, Daniels G, et al: Progression-free survival and biomarker correlates of response with bempeg plus nivo in previously untreated patients with metastatic melanoma: Results from the PIVOT-02 study. 2020 Society for Immunotherapy of Cancer Annual Meeting. Abstract 420. Presented November 11, 2020.
2. Diab A, Curti B, Bilen M, et al: REVEAL: Phase 1 dose-escalation study of NKTR-262, a novel TLR7/8 agonist, plus bempegaldesleukin: Local innate immune activation and systemic adaptive immune expansion for treating solid tumors. 2020 Society for Immunotherapy for Cancer Annual Meeting. Abstract 368. Presented November 11, 2020.
