

The ASCO Post is pleased to continue this occasional special focus on the worldwide cancer burden. In this issue, we feature a close look at the cancer incidence and mortality rates in Cameroon. The aim of this special feature is to highlight the global cancer burden for various countries of the world. For the convenience of the reader, each installment will focus on one country from one of the six regions of the world as defined by the World Health Organization (ie, Africa, the Americas, Southeast Asia, Europe, Eastern Mediterranean, and Western Pacific). Each section will focus on the general aspects of the country followed by the current and predicted rates of incidence and cancer-related mortality. It is hoped that through these issues, we can increase awareness and shift public policy and funds toward proactively addressing this lethal disease on the global stage.

Premila Leiphrakpam, MBBS, PhD

Chandrakanth Are, MBBS, MBA, FRCS, FACS
Cameroon is a lower-income country in Central Africa located along the Atlantic Ocean and neighbored by the Central African Republic, Chad, the Republic of the Congo, Equatorial Guinea, Gabon, and Nigeria.1 The country is ethnically diverse, with an estimated population of more than 31 million in 2024 (Table 1). The median age in Cameroon is 19 years, and approximately 45% of the Cameroon population is younger than age 15, with 17% being younger than age 5. The age group of between 5 and 64 years comprises 30% of the population, with only 4% of the population older than age 64.2 This is due to the decades-long effort to reduce the mortality rate among those younger than age 5 and the country’s ongoing high fertility rate.2
Cameroon remains one of the lowest-resource countries in Africa. In 2014, approximately two of five people (37.5%) lived below the poverty line in the country, and the rate is higher in rural areas (56.8%).3,4
Health Care
For the year 2023 to 2024, the national health-care budget of Cameroon ranged between 3.44% and 3.83% of the total national budget.5 This is lower than the commitment made by African leaders during the World Health Organization (WHO) Abuja Summit in April 2001 to allocate 15% of the annual budget to the health sector.6
Access to health care in Cameron is ineffective due to cost, distance, and lack of quality health information.3 Less than 3% of the population is covered by some type of health insurance–related mechanism,3 and about 67% of the health-care costs are paid out of pocket by households, according to the World Bank estimates in 2021.7
Cancer Profile
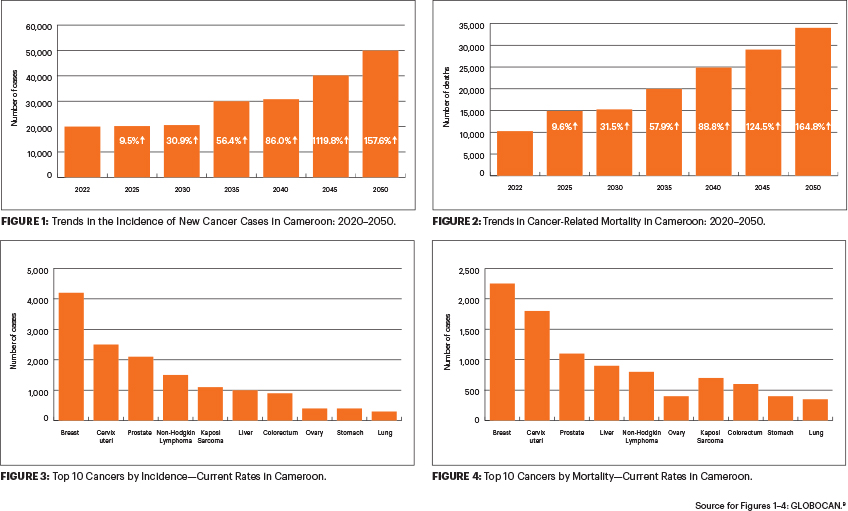
Cancer is a public health concern in Cameron, with a mortality-to-incidence rate greater than 65%.8 According to the WHO GLOBOCAN 2022 data, there were an estimated 19,564 new cases (Figure 1) and 12,798 cancer-related deaths in Cameroon (Figure 2).9 Citizens older than age 15 remain the most affected population, and pediatric cancers account for 1% to 2% of all cancers. Approximately 90% of patients with cancer seek treatment at the advanced stages of the disease for various reasons, and this contributes to the country’s high rate of cancer-related mortality.8
Breast cancer is the most frequently diagnosed cancer in Cameroon, with approximately 4,207 new cases reported in 2022 according to the WHO data. Breast cancer is followed by cervical cancer (2,525 new cases), prostate cancer (2,050 new cases), non-Hodgkin lymphoma (1,480 new cases), and Kaposi sarcoma (1,148 new cases), as shown in -Figure 3.9 Breast cancer is also the leading cause of cancer--related death in Cameroon, with 2,285 deaths reported in 2022. Breast cancer is followed by cervical cancer (1,837 deaths), prostate cancer (1,131 deaths), liver cancer (910 deaths), and non-Hodgkin lymphoma (834 deaths), as shown in Figure 4.9
At the current rate, without optimal intervention, the numbers of new cancer cases and cancer-related deaths are expected to rise by more than 158% and 165% by 2050 (50,389 new cases and 33,884 deaths, respectively).9 This epidemiologic shift in the number of new cancer cases has been attributed to the following factors: (1) persistence of infectious diseases–related cancers such as human papillomavirus (HPV), hepatitis B virus (HBV), hepatitis C virus (HCV), and Helicobacter pylori; (2) lifestyle modifications such as a sedentary lifestyle, unbalanced diet, smoking, alcohol consumption, and obesity; (3) exposure to harmful radiation such as radon; and (4) genetic factors.8
Cancer Control Initiatives
In response to the increasing cancer burden in Cameroon, the Ministry of Public Health created the National Committee for the Fight Against Cancer (NACFAC) in 1990. It was reorganized in 2002 with an overall objective to reduce cancer-related morbidity and mortality in Cameroon.8,10 The National Cancer Control Program was established in 2002 and was followed by the opening of cancer registries in Yaoundé and Douala in 2003.3
In 2019, NACFAC developed the 2020–2024 National Strategic Plan for Prevention and Cancer Control, a 5-year national strategic plan with the aim to reduce cancer-related morbidity and mortality by at least 10% by 2024 and attenuate its socioeconomic impact on the development of the country.8 To enhance awareness for the primary prevention of cancer in Cameroon, NACFAC organized sensitization campaigns for the general public during special days and events, such as during the month of October (“Octobre Rose”). Civil society organizations also organized sensitization campaigns within the community, professional, and academic settings.8
Although Cameroon does not have a national screening program for breast and cervical cancers, some public hospitals and private health services perform routine screening and
treatment of cervical cancer in some cities.8 The Cameroon Cervical Cancer Prevention Project ECHO (Extension for Community Health Care Outcomes) was launched in June 2018 and focused on cervical cancer education, promotion of HPV vaccination, screening and early detection, treatment of preinvasive and early-stage invasive cervical disease, and follow-up after treatment.11 The Mother-Daughter Approach to cervical cancer prevention is a model for expanding access and uptake of cervical cancer prevention services in Cameroon and has been ongoing since January 2022.12
Immunization against HBV is integrated into the routine Expanded Program on Immunization. A pilot phase to introduce the HPV vaccine for girls aged 9 to 13 was successfully completed in 2015 and has been included in the 2020–2024 National Strategic Plan for Prevention and Cancer Control (NCCP).8
Barriers to Cancer Control
Despite the increasing cancer burden, the paucity of reliable data due to the lack of an organized and effective cancer registry system is a major limiting factor in enhancing evidence-based decision-making for cancer control in Cameroon.10 Cameroon currently does not have a national screening program for breast and cervical cancers. Even though sporadic cancer screening campaigns were organized throughout the country, many of the precancerous lesions cannot be treated due to the lack of equipment.8 Insufficient human resources is another limiting factor for the management of cancer, with the availability of approximately 1 medical doctor and 8 nurses and midwives per 10,000 inhabitants in 2018. In addition, the lack of universal health care and high health-care costs; late presentation of cancer cases; and the impact of myths, misinformation, stigma, and sociocultural/religious beliefs on cancer education and awareness are some of the barriers to cancer control.10
The cancer control policies of the NCCP from 2004 to 2019 in Cameroon have been reported to have minimal impact on the following: the development of individual skills, strengthening of the community toward cancer prevention, and encouraging collaboration with other cancer control organizations and companies.13
Further Efforts to Improve Cancer Care
The 2020–2024 NCCP calls for the reduction of cancer morbidity and mortality by at least 10% by 2024. The main strategic components of the 5 year plan include: (1) increase awareness through health promotion to encourage behavior changes; (2) strengthen primary and secondary prevention with emphasis on the control of sexually transmitted diseases and to promote vaccination, screening, and early diagnosis of cancer; (3) upgrade the existing tertiary treatment centers, establish a national cancer institute, and decentralize cancer care; and (4) improve governance using the available resources.8
Given the significance of health promotion in cancer control and the role of community-based organizations and nongovernment organizations in promoting healthy lifestyles in populations, there is a need for the NCCP to establish firm collaboration with these organizations to strengthen their actions and expand services to all regions.
In addition, interventions to reduce the cancer burden should also focus on improving cancer surveillance and data at the national level, building and maintaining a skilled workforce, financing health-care insurance, reducing out-of-pocket health-care costs, and increasing the participation of stakeholders. With all these initiatives and the concerted efforts from various organizations, it is envisioned that, over time, Cameron will be prepared to tackle the rising cancer burden.
Dr. Leiphrakpam is Graduate Medical Education Research and Education Program Manager at the University of Nebraska Medical Center. Dr. Are is the Jerald L. & Carolynn J. Varner Professor of Surgical Oncology & Global Health; Associate Dean for Graduate Medical Education; and Vice Chair of Education Department of Surgery, University of Nebraska Medical Center, Omaha.
DISCLOSURE: Dr. Leiphrakpam reported no conflicts of interest. Dr. Are has a patent with the University of Nebraska Medical Center for a laparoscopy instrument.
REFERENCES
1. Central Intelligence Agency: The World Factbook. Cameroon. Available at https://www.cia.gov/the-world-factbook/countries/cameroon. Accessed November 25, 2024.
2. National Institute of Statistics and ICF. 2020: 2018 Cameroon Demographic and Health Survey, Yaounde, Cameroon, and Rockville, Maryland: NIS and ICF. Available at https://ins-cameroun.cm/wp-content/uploads/2022/05/ENG-00-00-Cameroon-DHS-2018-FINAL.pdf. Accessed November 25, 2024.
3. Republic of Cameroon, Ministry of Public Health (MINSANTE): Health Sector Strategy 2016–2027. Available at https://www.minsante.cm/site/?q=en/content/health-sector-strategy-2016-2027-0. Accessed November 25, 2024.
4. Republic of Cameroon: Ministry of Public Health (MINSANTE): 2020–2024. National Digital Health Strategic Plan. Available at https://www.minsante.cm/site/?q=en/content/2020-2024-national-digital-health-strategic-plan. Accessed November 25, 2024.
5. Republic of Cameroon, Ministry of Finance (MINFI): 2024 Finance Law: Report on the Nation’s Economic, Social, and Financial Situation and Prospects 2023 Financial Year. Available at https://minfi.gov.cm/en/2024-finance-law-report-on-the-nations-economic-social-and-financial-situation-and-prospects-2023-financial-year. Accessed November 25, 2024.
6. World Health Organization: The Abuja Declaration: Ten Years On (2010). Available at https://iris.who.int/handle/10665/341162. Accessed November 25, 2024.
7. World Health Organization Global Health Expenditure Database: Out-of-pocket expenditure (% of current health expenditure), Cameroon. Available at https://data.worldbank.org/indicator/SH.XPD.OOPC.CH.ZS?locations=CM. Accessed November 25, 2024.
8. Republic of Cameroon, Ministry of Public Health (MINSATE): 2020–2024 National Strategic Plan for Prevention and Cancer Control. Available at https://www.iccp-portal.org/system/files/plans/FINAL%20COPY%20OF%20PSNPLCa%20ENGLISH.pdf. Accessed November 25, 2024.
9. International Agency for Research on Cancer and World Health Organization: GLOBOCAN 2022. Available at https://gco.iarc.fr/en. Accessed November 25, 2024.
10. Mapoko BSE, Frambo A, Saidu Y, et al: Assessment of barriers to optimal cancer control in adult cancer treatment centres in Cameroon. Ecancermedicalscience 17:1601, 2023.
11. Fokom Domgue J, Pande M, Yu R, et al: Development, implementation, and evaluation of a distance learning and telementoring program for cervical cancer prevention in Cameroon. JAMA Netw Open 5:e2240801, 2022.
12. Elit L, Manjuh F, Kila L, et al: Mother-child approach to cervical cancer prevention in a low resource setting: The Cameroon Baptist Convention Health Services Story. Curr Oncol 31:3227-3228, 2024.
13. Abenwie SN, Tatiana M, Antaon JSSA, et al: Activities of the National Cancer Control Program in strengthening community action and developing individual skills for cancer prevention in Cameroon (2004–2019). Health Sci Dis 22:57-61, 2021.