

Colombia is located in the northwestern corner of South America, geographically privileged with coasts on both the Atlantic and Pacific Oceans, the Andean region, and the Amazon rainforest. Based on its population of nearly 50 million (see Table 1), Colombia is the second largest country in South America (after Brazil) and the third largest in Latin America (after Brazil and Mexico).
Life expectancy at birth is 76.6 years, with a median age of 31 years, and 80% of the population is urban. Important demographic changes that have taken place over the past century include increasing life expectancy, aging population, and a declining fertility rate. These demographic changes are associated with an increase in the population at risk of cancer and a growing demand for cancer prevention and treatment services.
GUEST EDITOR

Chandrakanth Are, MBBS, MBA, FRCS, FACS
Dr. Are is the Jerald L. & Carolynn J. Varner Professor of Surgical Oncology & Global Health; Associate Dean for Graduate Medical Education; and Vice Chair of Education Department of Surgery, University of Nebraska Medical Center, Omaha.
Over the past few decades, new sectors such as tourism, mining, and the manufacturing industry have grown to assume a larger role in the country’s economy, though petroleum and coffee continue to play a leading role. Colombia is classified in the upper-middle-income country group by the World Bank, and its health expenditure accounts for 7.22% of the gross domestic product.
Health-Care Policy in Colombia
Reformed in 1993, Colombia’s national health system is now centered around a Social Security Health System, which includes both contributory and subsidized plans that cover 95% of the population. The contributory plan is structured around the workforce (employees, independent workers, and pensioned adults), whereas the subsidized plan covers those below established household economic tiers and who cannot pay—representing 44% of the population. Cancer care is included in the benefit plans, and most basic treatments are covered.
Cancer Profile
Epidemiologic cancer reporting and tracking and the quality of cancer statistics in Colombia have improved significantly during the past half-century. The Death Certificate Registry is an important source of information related to mortality, as 93% of cancer deaths are properly and accurately captured.1
One of the oldest Latin American population-based cancer registries was developed in the city of Cali. It is an accurate and reliable source of data on local cancer incidence, mortality, and survival.2 Based on this experience, the Instituto Nacional de Cancerología (National Cancer Institute) sponsored the development of a population-based cancer registry, across five major cities, which has improved the availability of high-quality data on cancer statistics at the national level.
Table 1: General Facts About Colombia
|
Population |
49.1 million (July 2020) |
|
Median age |
31.2 years (2020) |
|
Population growth rate |
0.93% (2020) |
|
Birth rate |
15.4/1,000 population (2020) |
|
Death rate |
5.6/1,000 population (2020) |
|
Life expectancy at birth |
76.6 years (2020) |
|
Health expenditure |
7.2% of GDP (2017) |
|
Physicians |
2.1 physicians/1,000 population (2017) |
|
Hospital bed density |
1.7 beds/1,000 population (2017) |
|
Obesity prevalence rate |
22.3% (2016) |
|
Mobile telephones |
64.5 million (2018) |
|
Land lines |
7.0 million (2018) |
GDP = gross domestic product. Source: Central Intelligence Agency: The World Factbook—South America: Colombia. Available at https://www.cia.gov/library/publications/resources/the-world-factbook/geos/print_co.html. Accessed November 24, 2020.
In Colombia, cancer is the second leading cause of death in the general population after cardiovascular disease, and the leading cause of death for those between 30 and 69 years of age. In 2018, the estimated annual number of new cancer cases was 101,893, with 46,057 cancer-related deaths,3 ranking as an intermediate-level country in the global ranking of cancer incidence.
Stomach cancer remains the most common cause of cancer-related mortality for the whole population (Figure 1). As a result, there is significant ongoing research among Colombian investigators in this field. Geographic trends are prominent (in part linked to diet types), with the highest and lowest incidence of stomach cancer in the Andean region and Atlantic coast region, respectively.
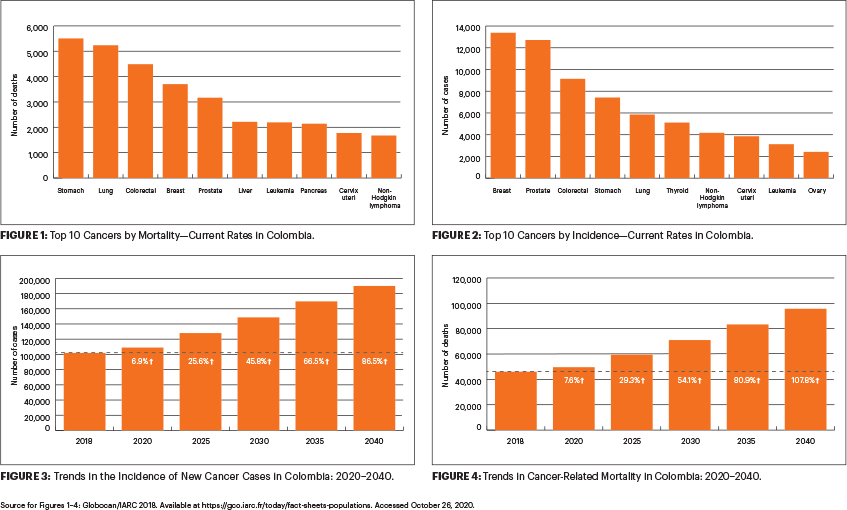
Figure 2 shows the top 10 cancers by incidence in Colombia. Among women, the top five causes of cancer in decreasing order are breast, colorectal, thyroid, cervical, and stomach cancers. In men, the top five cancers include those of the prostate, stomach, colorectum, lung, and lymphoma.
Recent studies analyzing the data from the past 2 decades have found a trend toward an increase in the incidence of colorectal and breast cancers, with a decrease in the incidence of stomach, lung, cervical, and prostate cancers.4,5 Additionally, studies derived from population-level cancer registries have shown a lower median survival in Colombia compared with that reported in the United States. These recent findings have led to efforts geared toward improving early diagnosis (via screening) and treatment as priorities at a national level.
Cancer Control Efforts
As part of these efforts, the Decennial Plan for Cancer Control (2012–2021), put forth by the government, established the policies, strategies, and priorities for cancer control in the country. This plan identified cancer as a public health problem and outlined six strategic lines for risk control focused on reducing risk factors for cancer, including smoking, alcohol, obesity, human papillomavirus (HPV), viral hepatitis B and C, and ultraviolet radiation exposure. Currently, the control of tobacco use, obesity prevention, and promotion of physical activity are active campaigns geared to reduce the incidence of cancer.
An important recent milestone has been the documented reduction in the mortality of patients with cervical cancer (from 14/100,000 in 1987 to 7.1/100,000 in 2018). The reasons behind this success are multifactorial and include a thorough evaluation of traditional screening methods, which subsequently allowed clinicians to improve the quality of screening and cytology. This was followed by implementation of a “see and treat” strategy for the more vulnerable population, screening with an HPV test, and the introduction of an HPV vaccine through the national immunization program. All of these initiatives were important steps undertaken to promote the primary and secondary prevention of cervical cancer.6,7 These efforts have been supported with research in cervical cancer across the country.
At this point, the government is preparing the next Decennial Plan for Cancer Control, slated to start in 2022. It is hoped that, through these sustained efforts supported by the government and cancer care professionals, Colombia will be able to address the rising national cancer burden adequately (Figures 3 and 4 on page 101).
DISCLOSURE: Dr. Guevara and Ms. Craig reported no conflicts of interest. Dr. Anaya is a consultant with Roche Diagnostics; and receives research funds from DNAtrix Therapeutics. Dr. Are is a board member with Global Laparoscopy Solutions Inc; has received research funding from Pfizer; and has a patent with the University of Nebraska Medical Center for a laparoscopy instrument.
REFERENCES
1. Cendales R, Pardo C: Quality of death certification in Colombia. Colomb Med (Cali) 49:121-127, 2018.
2. Bravo LE, García LS, Collazos P, et al: Reliable information for cancer control in Cali, Colombia. Colomb Med (Cali) 49:23-34, 2018.
3. World Health Organization, International Agency for Research on Cancer: Cancer today. Available at https://gco.iarc.fr/today/home. Accessed November 13, 2020.
4. Bravo LE, Muñoz N: Epidemiology of cancer in Colombia. Colomb Med (Cali) 49:9-12, 2018.
5. Piñeros M, Gamboa O, Hernández-Suárez G, et al: Patterns and trends in cancer mortality in Colombia 1984–2008. Cancer Epidemiol 37:233-239, 2013.
6. Muñoz N, Bravo LE: Epidemiology of cervical cancer in Colombia. Colomb Med (Cali) 43:298-304, 2012.
7. Vorsters A, Bosch FX, Bonanni P, et al: Prevention and control of HPV infection and HPV-related cancers in Colombia—A meeting report. BMC Proc 14(suppl 9):8, 2020.
Dr. Guevara is Professor of Surgery at the Universidad Nacional de Colombia, Instituto Nacional de Cancerologia, Bogota, Colombia. Ms. Craig is Research Support Specialist at Cornell University, Ithaca, New York. Dr. Are is the Jerald L & Carolynn J. Varner Professor of Surgical Oncology & Global Health; Associate Dean for Graduate Medical Education; and Vice Chair of Education Department of Surgery, University of Nebraska Medical Center, Omaha. Dr. Anaya is Professor and Chief of GI Surgery and Head of the Hepatobiliary Section, Department of GI Oncology at the Moffitt Cancer Center, Tampa.