


In a breakthrough proposal announced on July 8, the Centers for Medicare & Medicaid Services (CMS) plans to reimburse physicians for end-of-life counseling, a move that the oncology community has long been lobbying for. Arriving just as the presidential election cycle begins to heat up, the CMS proposal will ostensibly settle the infamous “death panel” debate that raged before the passage of the Affordable Care Act. A final decision will be made on November 1, and the proposal—if passed as expected—will take effect on January 1, 2016.
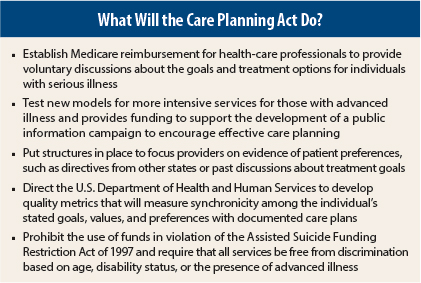
Although the CMS proposal was the result of exhaustive lobbying by major health-care organizations, it needed the imprimatur of policymakers, which came by way of a bill called the Care Planning Act of 2015, S. 1549, sponsored by U.S. Senators Johnny Isakson (R-GA) and Mark R. Warner (D-VA). The bill creates a Medicare benefit for patient-centered care planning for people with serious illnesses such as cancer. Medicare will reimburse health-care professionals for providing voluntary, structured discussions about the patient’s goals, illness, and treatment options.
Respecting Patient Preferences
Regarding the heated controversy over the so-called death panels and other fierce rhetoric that had long stalled this initiative, one of the bill’s authors, Senator Warner commented during a press conference:
In the past several years, some have deliberately chosen to misrepresent the purpose of care planning services to frighten people and to score cheap political points. It’s about making sure that your doctors, your hospital, and your family know what choices you have made about your care. If a patient prefers to explore every possible treatment option, that choice will be respected. And if an individual prefers a different approach after informed consultations with their health team, their family, and others, those choices should be documented and honored too. The important thing is being able to make that decision and trust that it will be respected.
Speaking with The ASCO Post, nationally regarded health-care expert Diana Mason, PhD, RN, FAAN, President of the American Academy of Nursing, said:
The proposed changes to the Medicare physician payment policy that would provide reimbursement for advance care planning services are important to improving end-of-life care. Encouraging and supporting health professionals in having end-of-life conversations with patients and their families is crucial if we are to respect patients’ goals and preferences for end-of-life care. This includes helping patients and their families to think about their preferences, complete advance directives, and be comforted knowing that their health-care providers understand their wishes. It also will help the health professionals to better understand and advocate for the patient’s preferences.”
Billing Concerns
To enable billing for these services, CMS has suggested the use of two new American Medical Association (AMA)-generated CPT codes (99479 and 99498), which allow providers to be reimbursed for their consultation in end-of-life conversations and also to encourage conversations prior to their being clinically necessary. The AMA codes are structured to cover substantive discussions about goals of care, treatment options, values, and preferences when it comes to end-of-life planning.
While feeling this is a step in the right direction, Dr. Mason noted, “I’m concerned that the conversation may have to be linked to a terminal diagnosis. The proposed rule says that the two CPT codes for advance planning services can be used ‘when the described service is reasonable and necessary for the diagnosis or treatment of illness or injury.’ We don’t always know when death is around the corner. These conversations should be part of an initial or periodic visit to a qualified health professional and all professionals should encourage and help patients to complete and properly file advance directives.”
Prior to the CMS proposal, certain private insurers had offered reimbursement. However, about three-quarters of the people who die each year in the United States are 65 and older, making Medicare the largest insurer at the end of life. Speaking from the perspective of a private payer, Lee N. Newcomer, MD, MHA, Senior Vice President, Oncology, Genetics and Women’s Health, UnitedHealthcare, said, “I applaud CMS for this change. End-of-life counseling is a difficult task—it takes time, emotional involvement, and courage for the patient and the physician. It’s only fair to compensate a physician for the hardest clinical encounter of his/her day. I don’t consider this payment as a mandate for end-of-life counseling, but it does remove one of the significant barriers preventing those discussions.”
Proponents of end-of-life counseling have contended that the focus on person-centered care and the longitudinal view of the care chain logically should include professional counseling and discussions on end-of-life options, which could lead to better informed choices by the dying, as well as lessened anxieties for families and caregivers.
Central to Quality Care
According to nationally regarded palliative care expert Eduardo Bruera, MD, FAAHPM, of The University of Texas MD Anderson Cancer Center, reimbursement for cognitive services such as end-of-life counseling is central to quality care. “ It is very important for CMS and all other payers to reimburse physicians for delivering end-of-life counseling. This is a medical procedure not different from a biopsy or a prescription for chemotherapy. It requires an appropriate physical setting, time, and a trained physician to conduct this medical procedure successfully.”
Moreover, Dr. Bruera sees the move by CMS as part of an important change in the medical culture. “It is very important that all graduate clinical programs in oncology conduct formal clinical training on how to safely conduct these interventions. Mandatory rotations in supportive and palliative care for all trainees will empower future oncologists to be successful at end-of-life counseling as well as multiple other interventions capable of reducing physical and psychosocial distress among advanced cancer patients.” He added, “This training will also reduce distress that can lead to burnout among cancer specialists.”
The oncology community has roundly approved this long-awaited move by CMS. Many view the proposed change as one more step in recognizing the difficult cognitive services that oncologists have been performing for decades without being reimbursed.
As Dr. Bruera pointed out, cognitive services are medical services. And the evidence has been there for a long time. For instance, a 2010 Journal of Clinical Oncology study1 concluded, “Patients with cancer are more likely to receive [end-of-life] care that is consistent with their preferences when they have had the opportunity to discuss their wishes for [end-of-life] care with a physician.” ■
Disclosure: Drs. Mason and Bruera reported no potential conflicts of interest. Dr. Newcomer is an employee and shareholder of UnitedHealthcare.
Reference
1. Mack JW, Weeks JC, Wright AA, et al: End-of-life discussions, goal attainment, and distress at the end of life. J Clin Oncol 28:1203-1208, 2010.