
GUEST EDITORS
Dr. Abutalib is Assistant Director, Hematology and Hematopoietic Cell Transplantation; Director, Hematopoietic Cell Transplant Apheresis Service, Cancer Treatment Centers of America, Zion, Illinois; Founder and Co–Editor-in-Chief, Advances in Cell & Gene Therapy. Dr. Medeiros is Professor and Chair, Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston.The ASCO Post is pleased to present Hematology Expert Review, an ongoing feature that quizzes readers on issues in hematology. In this installment, Drs. Abutalib and Medeiros explore the recently updated World Health Organization (WHO) classification of hematopoietic and lymphoid tissue malignancies, focusing on polycythemia vera. For each question that follows, select the one best answer. The correct answers and accompanying discussions appear below.
Question 1
Which of the following patient(s) require a bone marrow biopsy to facilitate the diagnosis of polycythemia vera?

Syed A. Abutalib, MD

L. Jeffrey Medeiros, MD
A. A male patient with JAK2 V617F mutation, hemoglobin of 13.5 g/dL, and subnormal serum erythropoietin level
B. A male patient with JAK2 V617F mutation, hemoglobin of 16.5 g/dL, and subnormal serum erythropoietin level
C. A patient with JAK2 V617F mutation, hemoglobin of 18.5 g/dL, and subnormal serum erythropoietin level
D. A and B are correct
Question 2
Which of the following is a minor criterion to facilitate the diagnosis of polycythemia vera?
A. Elevated hematocrit of > 48% in women and > 49% in men
B. Elevated hemoglobin of > 16.0 g/dL in women and > 16.5 g/dL in men
C. Bone marrow biopsy showing age-adjusted hypercellularity with panmyelosis and pleomorphic mature megakaryocytes
D. Subnormal serum erythropoietin level
Question 3
Which of the following is a well-described bone marrow characteristic of polycythemia vera?
A. Unilineage erythroid hyperplasia
B. Age-adjusted hypercellularity
C. Pleomorphic immature megakaryocytes
D. All of the above
Question 4
Which of the following morphologic features (in initially performed bone marrow biopsy) distinguishes polycythemia vera from essential thrombocythemia?
A. Panmyelosis
B. Negligible iron deposition
C. Increased reticulin fibrosis
D. All of the above
Answers to the quiz appear below.
Answers to Hematology Expert Review Questions
Question 1
Which of the following patient(s) require a bone marrow biopsy to facilitate the diagnosis of polycythemia vera?
Correct answer: D. A male patient with JAK2 V617F mutation, hemoglobin of 13.5 g/dL, and subnormal serum erythropoietin level and a male patient with JAK2 V617F mutation, hemoglobin of 16.5 g/dL, and subnormal serum erythropoietin level.
Expert Perspective
Laboratory studies that facilitate the diagnosis of polycythemia vera include detection of JAK2 V617F or functionally similar mutations (eg, JAK2 exon 12 mutations) and subnormal erythropoietin levels.1-4 Although JAK2 mutation occurs in more than 95% of patients with polycythemia vera, it is not specific for this entity: it is found in other myeloproliferative neoplasms and is also observed in a small subset (< 5%) of patients with acute myeloid leukemia, myelodysplastic syndromes, chronic myelomonocytic leukemia, and other myeloid malignancies.1,3,5-7 Functionally similar mutations in exon 12 of JAK2 are found in about 3% of polycythemia vera cases, which generally show a predominant erythroid hematopoiesis.1,2,8,9
It is important to emphasize that some patients may initially present with prominent thrombocytosis, as well as JAK2 V617F mutation and lower-than-expected hemoglobin levels and hematocrits, clinically mimicking essential thrombocythemia at the onset (ie, “masked polycythemia vera”). Such a group of patients may be unmasked sooner with diagnostic bone marrow showing histopathology characteristic of polycythemia vera.10-12 Therefore, determination of JAK2 mutation status alone (without bone marrow morphologic examination) is insufficient to distinguish polycythemia vera from JAK2-mutated essential thrombocythemia.6 Nonetheless, a diagnostic bone marrow biopsy may not be required, in patients with a sustained hemoglobin level of more than 18.5 g/dL in men (or > 16.5 g/dL in women) and a hematocrit of more than 55.5% in men (or > 49.5% in women), in the presence of JAK2 V617F or JAK2 exon 12 mutation and subnormal serum erythropoietin level1 (Table 1).
Question 2
Which of the following is a minor criterion to facilitate the diagnosis of polycythemia vera?
Correct Answer: D. Subnormal serum erythropoietin level.
Expert Perspective
Subnormal serum erythropoietin level is the only minor criterion to facilitate the diagnosis of polycythemia vera. Proper diagnosis of polycythemia vera requires three major criteria or the first two major criteria plus the minor criterion, as shown in Table 1.1
Question 3
Which of the following is a well-described bone marrow characteristic of polycythemia vera?
Correct Answer: B. Age-adjusted hypercellularity.
Expert Perspective
In polycythemia vera, the bone marrow biopsy shows age-adjusted hypercellularity with trilineage growth (panmyelosis), including prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic (differences in size), mature megakaryocytes1 (Figures 1 and 2).
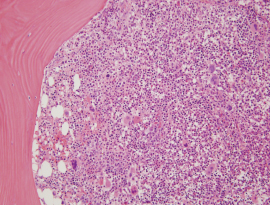
A markedly hypercellular (~ 95%) bone marrow for a 46-year-old man with polycythemia vera. Even at this low-powered magnification (hematoxylin-eosin stain, 200×), many mature megakaryocytes of different sizes (pleomorphism) can be seen.
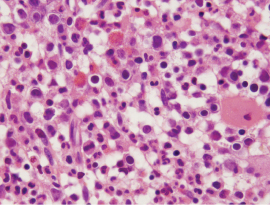
Under oil magnification (hematoxylin-eosin stain, 1,000×), the bone marrow shows panmyelosis with increased granulocytic and erythroid precursors showing maturation. One megakaryocyte is also present in this field without a relevant maturation defect.
Question 4
Which of the following morphologic features (in initially performed bone marrow biopsy) distinguishes polycythemia vera from essential thrombocythemia?
Correct Answer: D. All of the above.
Expert Perspective
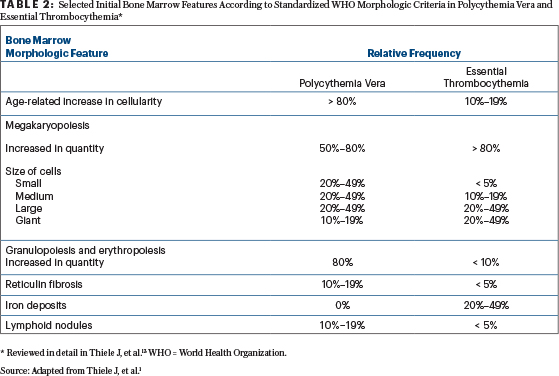
Using standardized bone marrow features, several groups have identified histologic patterns that are characteristic of the WHO-defined polycythemia vera, including so-called masked polycythemia vera.1,12,13-15 Erythropoiesis is usually normoblastic, erythroid precursors form large islets or sheets, and granulopoiesis is morphologically normal.1 Megakaryocytes are increased in number (particularly in cases with an excess of platelets) and frequently display hypersegmented nuclei. Cases with high platelet counts and low hemoglobin or hematocrit values may mimic essential thrombocythemia at the onset.1,11,12,16
Reticulin staining reveals a normal reticulin fiber network in about 80% of cases, but the remainder may display increased reticulin fibrosis and even mild-to-moderate collagen fibrosis, depending on the stage of disease at initial diagnosis.1,10-15,17,18 Even a minor increase in reticulin fibers (reticulin grade 1) at initial presentation of polycythemia vera has been associated with a more rapid progression to post– polycythemia vera myelofibrosis, underscoring the value of bone marrow biopsy1,13,17 (Figure 3).
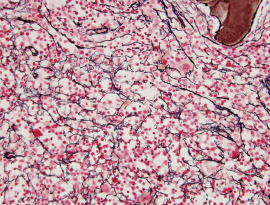
Reticulin stain of the bone marrow (400×) shows mildly increased fibrosis (myelofibrosis 1). Increased bone marrow reticulin fibrosis occurs in about 20% of cases of polycythemia vera and correlates with an increased risk of subsequent progression to post–polycythemia myelofibrosis.
Reactive nodular lymphoid aggregates are found in as many as 20% of cases.1,19 In more than 95% of cases, stainable iron is absent in bone marrow aspirate and biopsy specimens1,14,20 (Table 2). ■
DISCLOSURE: The authors reported no conflicts of interest.
REFERENCES
1. Thiele J, et al: Polycythemia vera, in Swerdlow SH, et al (eds): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, pp 39-43. Lyon, France, IARC, 2017.
2. Pardanani A, et al: Prevalence and clinicopathologic correlates of JAK2 exon 12 mutations in JAK2V617F-negative polycythemia vera. Leukemia 21:1960-1963, 2007.
3. Tefferi A, et al: Survival and prognosis among 1545 patients with contemporary polycythemia vera. Leukemia 27:1874-1881, 2013.
4. Mossuz P, et al: Diagnostic value of serum erythropoietin level in patients with absolute erythrocytosis. Haematologica 89:1194-1198, 2004.
5. Tefferi A: Novel mutations and their functional and clinical relevance in myeloproliferative neoplasms: JAK2, MPL, TET2, ASXL 1, CBL, IDH and IKZF1. Leukemia 24:1128-1138, 2010.
6. Tefferi A, et al: Long-term survival and blast transformation in molecularly annotated essential thrombocythemia, polycythemia vera, and myelofibrosis. Blood 124:2507-2513, quiz 2615, 2014.
7. Steensma DP, et al: The JAK2 V617F activating tyrosine kinase mutation is an infrequent event in both “atypical” myeloproliferative disorders and myelodysplastic syndromes. Blood 106:1207-1209, 2005.
8. Lakey MA, et al: Bone marrow morphologic features in polycythemia vera with JAK2 exon 12 mutations. Am J Clin Pathol 133:942-948, 2010.
9. Scott LM, et al: JAK2 exon 12 mutations in polycythemia vera and idiopathic erythrocytosis. N Engl J Med 356:459-468, 2007.
10. Barbui T, et al: Discriminating between essential thrombocythemia and masked polycythemia vera in JAK2 mutated patients. Am J Hematol 89:588-590, 2014.
11. Gianelli U, et al: The significance of bone marrow biopsy and JAK2V617F mutation in the differential diagnosis between the “early” prepolycythemic phase of polycythemia vera and essential thrombocythemia. Am J Clin Pathol 130:336-342, 2008.
12. Thiele J, et al: Initial polycythemia vera with thrombocytosis mimicking essential thrombocythemia. Acta Haematol 113:213-219, 2005.
13. Thiele J, et al: Diagnostic impact of bone marrow histopathology in polycythemia vera. Histol Histopathol 20:317-328, 2005.
14. Thiele J, et al: Bone marrow histopathology in the diagnosis of chronic myeloproliferative disorders: A forgotten pearl. Best Pract Res Clin Haematol 19:413-437, 2006.
15. Barbui T, et al: Masked polycythemia vera: Results of an international study. Am J Hematol 89:52-54, 2014.
16. Kvasnicka HM, et al: Prodromal myeloproliferative neoplasms: The 2008 WHO classification. Am J Hematol 85:62-69, 2010.
17. Abdulkarim K, et al: The impact of peripheral blood values and bone marrow findings on prognosis for patients with essential thrombocythemia and polycythemia vera. Eur J Haematol 86:148-155, 2011.
18. Thiele J, et al: European consensus on grading bone marrow fibrosis and assessment of cellularity. Haematologica 90:1128-1132, 2005.
19. Barbui T, et al: Initial bone marrow reticulin fibrosis in polycythemia vera exerts an impact on clinical outcome. Blood 119:2239-2241, 2012.
20. Ellis JT, et al: Studies of the bone marrow in polycythemia vera and the evolution of myelofibrosis and second hematologic malignancies. Semin Hematol 23:144-155, 1986.