
A Century of Progress
The text and photograph on this page are excerpted from a four-volume series of books titled Oncology Tumors & Treatment: A Photographic History, by Stanley B. Burns, MD, FACS. The photo below is from the volume titled “The Antiseptic Era: 1876–1900” by Stanley B. Burns, MD, FACS, and Elizabeth A. Burns. The photograph appears courtesy of Stanley B. Burns, MD, and The Burns Archive. To view additional photos from this series of books, visit burnsarchive.com.
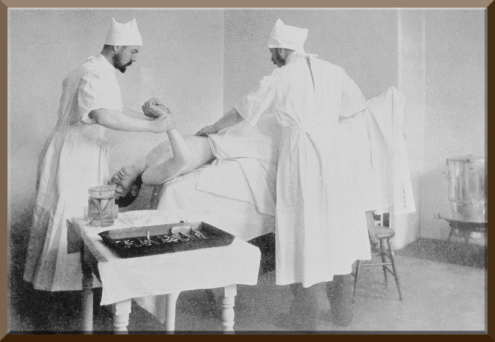
During the 1890s, aseptic principles were extended only to the operative area of the patient, not the surgeon, although some surgeons did advocate the use of special white or colored uniforms, and hand washing had already been established. In 1895, just 7 years after Arpad Gerster, MD, published his text on asepsis, which included some aseptic techniques, New York surgeon Carl Beck, MD, published A Manual of Surgical Sepsis. In it, he demanded a full-body white coverall suit with a hat for the patient and a white gown and a hat for the physicians. Drs. Gerster and Beck were both associated with German Hospital (now known as Lenox Hill Hospital).
The Advent of Anesthesia
The advent of anesthesia permitted the long procedures inherent in major cancer surgery to proceed uninterrupted. Although the pain had been removed, resuscitation due to respiratory or cardiac arrest from blood loss, shock, or the anesthetic itself was often necessary. This photograph documents the resuscitation of a patient on the operating table. Dr. Beck describes his procedure, which at the time was on the cutting edge of medical knowledge:
Many deaths during or after operations, from what is vaguely termed ‘shock,’ are doubtless closely related to the effects of anesthetics.... If respiration becomes impaired, operations may properly be finished without the further administration of the anesthetic. It is less cruel to trouble the patient and to save his life than to give him the so-called benefits of full anesthesia and to risk his life under the pretext of humanity.
The forceps with which the tongue is drawn forward merits some attention. Whenever the symptoms of respiratory impediment appear and do not yield promptly, the assistant in charge of the anesthetic should place his fingers behind the angle of the lower jaw and force the jaw forward. If breathing does not then promptly become normal, the tongue must be seized with sterilized forceps and be pulled forward... the handles be provided with a catch, so that the instrument cannot slip from the tongue.... The introduction of the forceps is frequently difficult, as the teeth may be pressed firmly together, in which case the Roser-Konig mouth forceps is of great value, as it rapidly separates the maxillae.... If ordinary means do not suffice to restore breathing, resort must be had to the induction of artificial respiration. The writer has found it useful to combine artificial respiration with stimulation of the heart and lowering of the head....
After having placed the patient in a position similar to that of the Trendelenburg, an assistant grasps the arms at the elbows, carries them outward and upward above the head, and brings them back to the anterior surface of the thorax. This movement should be performed in a rhythmical manner and about eighteen times per minute. At the same time another assistant thrusts his fingers against the apex of the heart, as if employing a species of massage. While these manipulations are being made camphorated oil and tincture of strophanthus may be injected hypodermically. Many other valuable methods exist but it is best to stick to a few so as to become thoroughly familiarized with them and carry them out well.
[Dr. Beck noted the differences in the potential of anesthetics to cause shock and death.] The majority of deaths under chloroform anesthesia occur at the preliminary stage before the surgeon can use the knife.... The dangers of ether anesthesia usually set in during its after-effect.... Oedema pulmonum, bronchopneumonia, and collapse, according to a number of reliable surgeons, have frequently followed the administration of ether.... Collapse may take place even several hours after the operation and is then generally not attributed to the anesthesia…. It is natural that erroneous conclusions are drawn in reference to the ‘safety’ of ether.... The dangers of chloroform appear more formidable to the practitioner, who dreads a fatal collapse in the operating room more than he does one in the sick-bed—that is, after some time has elapsed following the operation; therefore he gives preference to ether.”
A Different Resuscitative Procedure
At Johns Hopkins Hospital, a different operative resuscitative procedure was described the year before in its hospital journal. One major difference between the two techniques was that Hopkins recommended the assistant stand on the operative table and hold the patient at a greater angle to facilitate pulmonary drainage. By the end of the second decade of the 20th century, several of modern anesthesia’s safety precautions had been implemented, and surgery became significantly safer. ■