

Women were more likely to have breast cancer that was overdiagnosed than to have earlier detection of a tumor that was destined to become large.— H. Gilbert Welch, MD, and colleagues
Tweet this quote
In a study using Surveillance, Epidemiology, and End Results (SEER) data reported in The New England Journal of Medicine, H. Gilbert Welch, MD, of Dartmouth Institute for Health Policy and Clinical Practice, and colleagues found that screening mammography has resulted in a substantial increase in the detection of small breast tumors, many of which represent overdiagnosis, accompanied by only a modest decrease in the detection of larger breast tumors.1 Their analysis also indicated that the reduction in breast cancer mortality after implementation of screening is mainly the result of improved systemic therapy.
Study Details
In the analysis, SEER data from 1975 through 2012 were used to calculate the tumor-size distribution and tumor size–specific incidence of breast cancer among women aged ≥ 40 years. Tumor size–specific cancer case fatality rates over 10 years were examined for two time periods: a baseline period before the implementation of widespread screening mammography (1975–1979) and a period including the most recent years, for which 10 years of follow-up data were available (2000–2002). The denominator for the case fatality rate was the number of women receiving a diagnosis of breast cancer at the beginning of a 10-year period, and the numerator was the number of deaths from breast cancer within 10 years after diagnosis.
Changes in Size Distribution
From 1975 to 2012, the proportion of tumors that were small (defined as invasive tumors measuring < 2 cm or in situ carcinomas) increased from 36% to 68%, and the proportion that were large (defined as invasive tumors measuring ≥ 2 cm) decreased from 64% to 32%. The change in size distribution was less related to any substantial decrease in the incidence of large tumors than to a sizable increase in the detection of small tumors. Compared with the era before widespread screening, the incidence of large tumors decreased by 30 cases of cancer per 100,000 women (from 145 to 115 cases/100,000) in the screening era. At the same time, the incidence of small tumors increased by 162 cases of cancer per 100,000 women (from 82 to 244 cases/100,000).
On the assumption that the true underlying incidence of clinically meaningful cancer has remained unchanged (based on the observation that the rates of metastatic disease at diagnosis have been steady for decades, despite screening), the data suggest that 30 cases of cancer/100,000 women would have become large but were detected earlier, and the remaining 132 cases of cancer per 100,000 women were overdiagnosed—ie, screening-detected cancer cases that never would have led to clinical symptoms.
Tumor Size–Specific Mortality Risk
Data on tumor size–specific 10-year risk of death from breast cancer show reduced risks for the 2000 to 2002 diagnosis cohort vs the 1975 to 1979 diagnosis cohort as follows (see Fig. 1): relative risk (RR) = 0.79 (95% confidence interval [CI] = 0.74–0.84) for ≥ 5.0 cm, 0.70 (95% CI = 0.65–0.75) for 3.0 to 4.9 cm, and 0.58 (95% CI = 0.53–0.62) for 2.0 to 2.9 cm among large tumors and RR = 0.38 (95% CI = 0.34–0.42) for 1.0 to 1.9 cm, 0.26 (95% CI = 0.21–0.32) for < 1.0 cm, and 0.47 (95% CI = 0.32–0.71) for in situ cancers. According to the investigators, the declining case fatality rate for large tumors predominantly reflected improved treatment. In contrast, the declining rate for small tumors was biased by the combined effects of lead time bias, length bias (overestimation of the duration of survival among women with screening-detected tumors), and overdiagnosis.
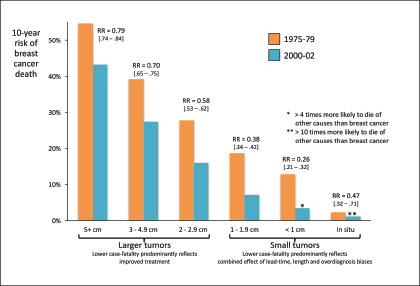
Fig. 1: 10-year risk of breast cancer death for 1975–1979 vs 2000–2002 in a SEER analysis. Courtesy of H. Gilbert Welch, MD.
In an analysis comparing survival rates with the general population, it was found that women with in situ carcinomas or invasive tumors < 1 cm in the 2000 to 2002 cohort had 10-year relative survival rates exceeding 100% vs age-matched women in the general population. As stated by the investigators: “In the period from 2000 through 2002, women with tumors < 1 cm in size were more than four times as likely to die from causes other than breast cancer than from breast cancer. In that same period, women with in situ carcinoma were more than 10 times as likely to die from causes other than breast cancer than from breast cancer.”
Effects of Screening and Improved Treatments
An analysis of the effect of improved treatment on breast cancer mortality had screening mammography not occurred indicated an estimated reduction of approximately 17 deaths per 100,000 women with tumors of 2.0 to ≥ 5.0 cm. The analysis of the effect of screening on mortality assumed that the reduction in the incidence of large tumors was attributable to screening and that the reduction directly translated to a reduction in mortality. The reduction in mortality associated with screening during the period of more recent therapy (2000–2002 cohort) was approximately 8 deaths per 100,000 women. Thus, improved treatment can be considered to be responsible for approximately 68% (17/25 [= 17 + 8]) of the reduction in breast cancer mortality.
As stated by the investigators: “The potential of screening to lower breast cancer mortality is reflected in the declining incidence of larger tumors. However, with respect to only these large tumors, the decline in the size-specific case fatality rate suggests that improved treatment was responsible for at least two thirds of the reduction in breast cancer mortality.”
The investigators concluded: “Although the rate of detection of large tumors fell after the introduction of screening mammography, the more favorable size distribution was primarily the result of the additional detection of small tumors. Women were more likely to have breast cancer that was overdiagnosed than to have earlier detection of a tumor that was destined to become large. The reduction in breast cancer mortality after the implementation of screening mammography was predominantly the result of improved systemic therapy.” ■
Disclosure: For full disclosures of the study authors, visit www.nejm.org.
Reference