

Syed A. Abutalib, MD

L. Jeffrey Medeiros, MD
GUEST EDITORS: Dr. Abutalib is Assistant Director, Hematology and Hematopoietic Cell Transplantation Director, Hematopoietic Cell Transplant Apheresis Service, Cancer Treatment Centers of America, Zion, Illinois, Editor-in-Chief, Advances in Cell & Gene Therapy. Dr. Medeiros is Professor and Chair, Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston.
Question 1
Which statement about epidemiology and clinical features is correct?
Correct answer: C. In addition to splenomegaly, bleeding from mucocutaneous surfaces or the gastrointestinal tract is reported in about 25% of CNL cases.
Expert Perspective
CNL is a rare type of myeloproliferative neoplasm, one of seven defined in the current WHO classification (Table 1). Similar to atypical CML, CNL usually affects older adults (Choice A is incorrect), and WHO-defined diagnostic criteria require exclusion of polycythemia vera, essential thrombocythemia, primary myelofibrosis, and CML (BCR-ABL1–positive) as well as absence of PDGFRA, PDGFRB, FGFR1, PCM1-JAK2, fusions (Choice B is incorrect).1 A history of bleeding from mucocutaneous surfaces or the gastrointestinal tract is reported in 25% to 30% of patients (Choice C is correct).1 Hepatosplenomegaly is common in patients with CNL.1 CNL lacks dysplastic features and has < 10% circulating immature myeloid cells1 (Figure 1).
_____________________________________________________________
TABLE 1: WHO CLASSIFICATION OF MYELOPROLIFERATIVE NEOPLASMS
- Chronic neutrophilic leukemia
- Chronic myeloid leukemia, BCR-ABL1–positive
- Essential thrombocythemia
- Polycythemia vera
- Primary myelofibrosis
- Chronic eosinophilic leukemia, not otherwise specified
- Myeloproliferative neoplasm, unclassifiable
Source: Bain BJ, et al.
_____________________________________________________________
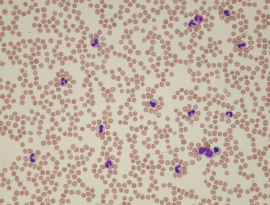
FIGURE 1: Characteristic neutrophilia in a peripheral blood smear.
Question 2
Which statement about microscopy is correct?
Correct answer: A. Segmented neutrophils plus banded neutrophils constitute ≥ 80% of the total white blood cells.
Expert Perspective
The microscopic aspects of the WHO diagnostic criteria for CNL are highlighted in Table 2 and Figures 1, 2, and 3. The peripheral blood monocyte count should be < 1 × 109/L.1 (Choice B is incorrect). Peripheral blood white blood cell count is ≥ 25 × 109/L1 (Choice C is incorrect).
_____________________________________________________________
TABLE 2: PERIPHERAL BLOOD AND BONE MARROW ON MICROSCOPIC EXAMINATION IN CNL ACCORDING TO WHO DIAGNOSTIC CRITERIA
Peripheral blood white blood cell count is ≥ 25 × 109/L
- Segmented neutrophils plus banded neutrophils constitute ≥ 80% of the white blood cells
- Myeloblasts are rarely observed
- Neutrophil precursors (promyelocytes, myelocytes, and metamyelocytes) constitute < 10% of the white blood cells
- Monocyte count < 1 × 109/L
- No dysgranulopoiesis
- Hypercellular bone marrow
- Neutrophil granulocytes increased in percentage and number
- Neutrophil maturation appears normal (no dysgranulopoiesis)
- Myeloblasts constitute < 5% of the nucleated cells
a Criteria rely on absolute or arbitrary values that may not reflect the biology of the disease (reviewed in detail by Dao et al2).
Source: Bain BJ, et al.1
CNL=chronic neutrophilic leukemia; WHO = World Health Organization.
_____________________________________________________________
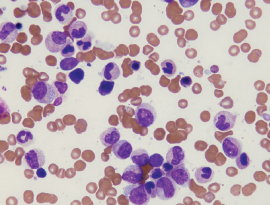
FIGURE 2: Bone marrow aspirate smear demonstrates neutrophil proliferation from myelocytes to segmented forms with toxic granulation but no other significant abnormalities.
Question 3
Which statement about genetic profiling is correct?
Correct answer: C. JAK2 V617F mutation may be present in CNL.
Expert Perspective
Conventional cytogenetic studies are normal in nearly 90% of CNL cases.1 There is no Philadelphia chromosome or BCR-ABL1 fusion in CNL (Choice A is incorrect). Cases with the neutrophilic variant of CML have a variant fusion BCR-ABL1, which encodes a p230 BCR-ABL 1 protein.1 CNL is known to be strongly associated with CSF3R mutation.1-4 (Choice B is incorrect; see in-depth review by Dao et al.2) JAK2 V617F has been reported in at least a dozen patients with CNL and is sometimes homozygous1,5 (Choice C is correct).
Question 4
Which statement about leukemoid reaction, plasma cell neoplasms, and t(15;19)(q13;p13.3) is correct?
Correct answer: C. Patients with CNL who have t(15;19)(q13;p13.3) may respond to imatinib therapy.
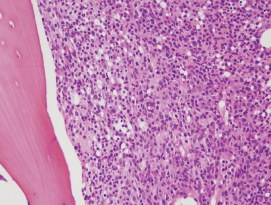
FIGURE 3: The bone marrow biopsy specimen is hypercellular, showing a markedly elevated myeloid-to-erythroid ratio, with increased numbers of neutrophils, particularly mature segmented forms.
Expert Perspective
Given the frequency of a neutrophilic leukemoid reaction in association with plasma cell myeloma and monoclonal gammopathy of undetermined significance, the bone marrow should be examined for evidence of a plasma cell neoplasm in all cases of suspected CNL.1,6 If a plasma cell neoplasm is present (and CSF3R T6181 or another activating CSF3R mutation is absent1), only then is demonstration of clonality of myeloid cells by cytogenetic or molecular studies advocated (Choice B is incorrect).1 Complete cytogenetic remission with imatinib was reported in a patient with CNL associated with t(15;19)(q13;p13.3), suggesting the possibility of an unidentified fusion gene in some cases of CNL1,7 (Choice C is correct).
Acknowledgment: Faiz Ahmed Hussain, MD, of the Department of Internal Medicine, Jackson Park Hospital, Chicago, assisted in preparing this review.
DISCLOSURE: Dr. Abutalib is on the advisory board of Juno Pharmaceuticals. Dr. Medeiros reported no conflicts of interest.
REFERENCES
1. Bain BJ, Brunning RD, Orazi A, et al: Chronic neutrophilic leukaemia, in Swerdlow SH, Campo E, Harris NL, et al (eds): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, pp 37-38. Lyon, France, International Agency for Research in Cancer, 2017.
2. Dao KT, Tyner JW, Gotlib J: Recent progress in chronic neutrophilic leukemia and atypical chronic myeloid leukemia. Curr Hematol Malig Rep 12:432-441, 2017.
3. Maxson JE, Gotlib J, Pollyea DA, et al: Oncogenic CSF3R mutations in chronic neutrophilic leukemia and atypical CML. N Engl J Med 368:1781-1790, 2013.
4. Pardanani A, Lasho TL, Laborde RR, et al: CSF3R T618I is a highly prevalent and specific mutation in chronic neutrophilic leukemia. Leukemia 27:1870-1873, 2013.
5. Mc Lornan DP, Percy MJ, Jones AV, et al: Chronic neutrophilic leukemia with an associated V617F JAK2 tyrosine kinase mutation. Haematologica 90:1696-1697, 2005.
6. Bain BJ, Ahmad S: Chronic neutrophilic leukaemia and plasma cell-related neutrophilic leukaemoid reactions. Br J Haematol 171:400-410, 2015.
7. Choi IK, Kim BS, Lee KA, et al: Efficacy of imatinib mesylate (STI571) in chronic neutrophilic leukemia with t(15;19): Case report. Am J Hematol 77:366-369, 2004.